TCAs and Thrombocytopenia?
Does anafranil affects blood platelets?
Anafranil (clomipramine) can indeed affect blood platelets. Here’s a detailed explanation:
Anafranil, a tricyclic antidepressant, has been associated with potential platelet-related effects:
- Thrombocytopenia Risk
- In rare cases, Anafranil can cause a decrease in platelet count (thrombocytopenia)
- This is considered an uncommon side effect
- Typically occurs in the early stages of treatment
- Platelet Aggregation
- Some studies suggest that tricyclic antidepressants like Anafranil may slightly alter platelet aggregation
- This can potentially impact blood clotting mechanisms
- Monitoring Recommendations
- Patients starting Anafranil should have baseline blood tests
- Periodic blood count monitoring is recommended, especially in the initial treatment phase
- Any unusual bruising or bleeding should be reported to a healthcare provider
- Clinical Significance
- Most patients do not experience significant platelet-related issues
- The risk is generally low but not zero
- Individual patient factors can influence potential side effects
Important Note: Always consult with a healthcare professional about specific medication concerns. They can provide personalized advice based on your individual health history and current medical conditions.
If you’re concerned about platelet effects, your doctor can perform blood tests to monitor your platelet count while on this medication.
Drug-Induced Thrombocytopenia (DITP) is a serious condition where certain medications cause a significant drop in platelet count. Here’s a comprehensive overview:
Definition:
- A condition where medications trigger an immune-mediated destruction of platelets
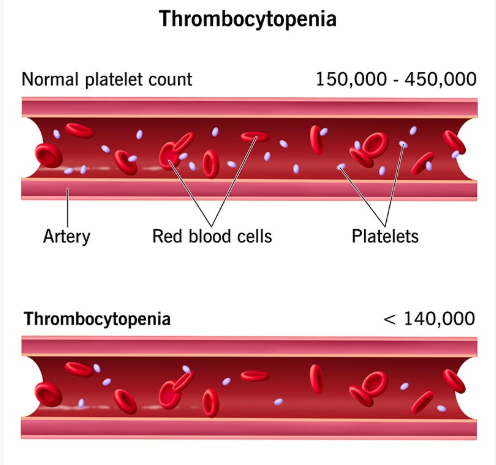
- Platelets are reduced below normal levels (typically <150,000 platelets/μL)
- Can occur within days to weeks after medication exposure
Mechanism:
- Immune-Mediated Destruction
- Drugs trigger antibody formation
- Antibodies target and destroy platelets
- Leads to rapid platelet count reduction
- Types of Reactions
- Immediate reaction (within days of drug exposure)
- Delayed reaction (can develop after prolonged use)
Common Medications Associated with DITP:
- Antibiotics (penicillins, sulfonamides)
- Anticonvulsants
- Quinine
- Heparin
- NSAIDs
- Certain psychiatric medications
- Sulfonylureas
- Some antiplatelet drugs
Clinical Manifestations:
- Unexplained bruising
- Petechiae
- Mucosal bleeding
- Prolonged bleeding time
- Potential severe hemorrhagic complications
Diagnosis:
- Detailed medication history
- Platelet count assessment
- Ruling out other thrombocytopenia causes
- Potential drug withdrawal challenge test
Management:
- Immediate drug discontinuation
- Supportive care
- Potential corticosteroids
- Platelet transfusion in severe cases
- Close medical monitoring
Prognosis:
- Usually reversible upon drug discontinuation
- Platelet count typically normalizes within days to weeks
- Avoid re-exposure to the causative medication
Warning Signs:
- Sudden unexplained bruising
- Excessive bleeding
- Rapid platelet count decline
- Seek immediate medical attention if these occur
Prevention:
- Comprehensive medication review
- Alert healthcare providers about previous DITP episodes
- Consider alternative medications
Treatment of Thrombocytopenia
Treatment for thrombocytopenia depends on the underlying cause and severity of the condition. Here are some common treatment options:
Medications
- Corticosteroids: Prednisone or dexamethasone may be prescribed to reduce platelet destruction and increase platelet production.
- Immunoglobulins: Intravenous immunoglobulin (IVIG) can be used to suppress the immune system and reduce platelet destruction.
- Rituximab: An antibody that targets B cells, which can help reduce platelet destruction in immune thrombocytopenic purpura (ITP).
- Thrombopoietin (TPO) stimulators: Eltrombopag (Promacta) and romiplostim (Nplate) can increase platelet production by stimulating the bone marrow.
- Antiplatelet agents: Aspirin and clopidogrel may be used to reduce platelet aggregation and prevent bleeding complications.
Surgical Intervention
- Splenectomy: Removing the spleen can increase platelet counts in some cases, especially for patients with chronic ITP.
- Bone marrow transplantation: In severe cases of aplastic anemia or myelodysplastic syndrome, bone marrow transplantation may be necessary.
Blood Transfusions
- Platelet transfusions: Used to treat life-threatening bleeding or to support patients undergoing surgery or other invasive procedures.
- Fresh frozen plasma (FFP) transfusions: May be used to treat bleeding complications, especially in patients with severe thrombocytopenia.
Other Therapies
- Phlebotomy: Regular blood draws can help reduce platelet destruction and increase platelet counts.
- Intravenous iron: May be used to treat iron deficiency anemia, which can contribute to thrombocytopenia.
- Supportive care: Patients with thrombocytopenia may require close monitoring and supportive care, including transfusions, to manage bleeding complications.
Important Considerations
- Cause-specific treatment: Treatment should be tailored to the underlying cause of thrombocytopenia.
- Individualized approach: Treatment plans should be individualized based on the patient’s age, overall health, and severity of thrombocytopenia.
- Monitoring: Regular monitoring of platelet counts and bleeding risk is essential to adjust treatment and prevent complications.
It’s essential to consult with a healthcare provider to determine the best course of treatment for thrombocytopenia based on the individual patient’s condition and needs.

