Are We All Schizophrenic? Delusions – Hallucinations
The ignorance in the public understanding of schizophrenia and related disorders is shockingly poor, with a survey by the National Alliance on Mental Illness indicating that 64% of Americans are unable to recognize its symptoms or incorrectly think the symptoms include split or multiple personalities. Misunderstanding schizophrenia is a key driver of the stigmatization of individuals with the condition, which has detrimental consequences, such as reduced housing and employment opportunities, diminished quality of life and health, low self-esteem, more symptoms and stress – which only further exacerbates the condition and reduces chances of recovery.
While misportrayal in the media and the name itself (schizo = split, phrenia = mind) are partly to blame, schizophrenia continues to be largely misunderstood as many of us think we are unable to relate. We are unable to put ourselves in the shoes of someone with the disorder. So let’s take the time now to set the record straight.
What you are about to discover is that we may be more able to relate to people that have experienced schizophrenic episodes than we think. Both new and not so new research reveals that the symptoms of schizophrenia are more common in non-schizophrenic individuals than we like to think.
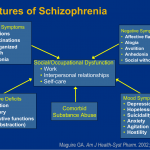
The first criteria in the DSM-V for a schizophrenia diagnosis lists five main symptoms, at least two of which must be present for at least one month. One of the two symptoms must be delusions, hallucinations or disorganized speech.
- Delusions
- Hallucinations
- Disorganized speech (e.g., frequent derailment or incoherence)
- Grossly disorganized or catatonic behavior
- Negative symptoms (i.e., diminished emotional expression or avolition)
Yet having only one symptom is sufficient for meeting symptom criteria if the delusions are considered bizarre (totally and utterly impossible, not understandable to same-culture peers and not derived from ordinary life experiences), or if auditory hallucinations involve a voice keeping up a running commentary of thoughts and behaviors or two or more voices talking with each other.
The key question is how common are these symptoms in the general populace? For the first part in the series we will consider delusions.
Symptom 1 – Delusions
Delusions are classified in the DSM-V as:
“…fixed beliefs that are not amenable to change in light of conflicting evidence. Their content may include a variety of themes (e.g. persecutory, referential, somatic, religious, grandiose)… The distinction between a delusion and a strongly held idea is sometimes difficult to make and depends in part on the degree of conviction with which the belief is held despite clear or reasonable contradictory evidence regarding its veracity.”
Have I ever had beliefs that I believed to be true despite conflicting evidence ? Or, although no proof against the truth of my belief can be found, did I believe with my mind, body and soul despite other people finding the idea implausible? Check! And have I ever had these beliefs persisting for a month or more? Check! Have I ever had schizophrenia or a related disorder? No.
A large body of evidence supports this idea, that we all have experienced non-pathological delusional beliefs throughout our lifetime and even generally in day to day life, and some delusions may actually be good for us (see the end of this article). For example one study found that over 10% of the non-clinical general population experience grandiose beliefs, i.e. that they are extraordinarily special in some way, although the belief is typically held with less conviction, less resistance to change and causes less significant social and occupational impairment than in those diagnosed with schizophrenia.
Professor of Clinical Psychology at Oxford University, Daniel Freeman, published a review of the literature in 2006 stating that:
“Approximately 1% to 3% of the nonclinical population have delusions of a level of severity comparable to clinical cases of psychosis. A further 5% to 6% of the nonclinical population have a delusion but not of such severity. Although less severe, these beliefs are associated with a range of social and emotional difficulties. A further 10% to 15% of the nonclinical population have fairly regular delusional ideation.”
Moreover, there is an inverse relationship between our age and how common and strongly held our delusional beliefs are. I don’t think anyone would argue that children are inherently delusional creatures: Magical, superstitious, bizarre, grandiose, paranoid and all kinds of delusions are not unusual for their rapidly developing yet immature belief systems.
Who here believed monsters lived under their beds or in the closet despite being shown repeatedly that there is nothing there? When I was around four or five, I believed I was a magical being that faeries had gifted sacred magical dust for super powers like flying off of the couch. I was so frustrated and furiously upset when no one would believe me that I tried to run away with the faeries, quite literally!
Similarly, delusional beliefs are pretty common in adolescents and young adults. In comparison to our previously mentioned grandiose delusions held by 10% of the general population, some studies have shown that the same beliefs are experienced by up to a colossal 75% of 15-26 year old’s. What’s more is that another study has shown that this subset of highly delusional individuals experience more distress and preoccupation associated with their delusional beliefs than the general population, as found in schizophrenia.
Interestingly, the extent to which a delusion is believed, how much it interferes with a person’s life and its emotional impact are what researchers often use to set pathological delusions apart from non-pathological ones, as these factors are typically more extreme in schizophrenic patients. If you can recall however:
“Approximately 1% to 3% of the nonclinical population have delusions of a level of severity comparable to clinical cases of psychosis.”
Herein lies the rub, “normal” and seemingly non-pathological delusions can be highly distressing, make you and perhaps others question your sanity and have huge emotional and life changing impacts.
Let’s say one day you have a profound religious experience where you believed that God was talking directly to you, reminding you of your sins or your importance and offering you a chance to repent by sending you on a personal mission. This is not an overwhelmingly uncommon experience in religious communities. You might believe in your mission to the core of your being, quit your job, feel overwhelmingly distressed, leave your family and friends despite their pleas, abandon everything and head off into the unknown on your religious mission.
Or let’s say that you less extravagantly “find God/Jesus”, believing that God/Jesus can hear you and is watching you and that you can influence real-life world events through praying to God/Jesus. This belief is not considered a delusion seeing as millions of other people believe the same – despite their being no way to conclusively prove this is true.
But if you replace God with the all-powerful Mars alien Lord Ziltoid, and there is not a group of individuals believing this too, it could easily be considered a pathological delusion. Unless you are a child of course, then we just chalk it down to an overactive imagination or a phase.
The same goes for non-religious beliefs that may or may not be considered delusional. For a little perspective, here are a few examples of common delusion themes, and a typical related question used in research-based diagnostic tools like the Peters et al. Delusions Inventory (PDI):
- Delusions of grandeur – Do you ever feel that you are a very special, unique or unusual person or are destined to be someone important?
- Delusions of control – Do you ever feel as if electrical devices such as computers can influence the way you think, or that there is a force, power or other people that can interfere with your thoughts or actions?
- Delusions of guilt – Do you ever feel that you have sinned more than the average person?
- Delusions of reference – Do you see any special meaning for yourself in everyday objects?
- Delusions of persecution – Do you ever feel there is a conspiracy against you?
- Delusion of jealousy or paranoia – Do you ever think that someone/your spouse is talking about you, hiding things from you or being unfaithful to you behind your back?
- Magical delusions – Do you believe in the power of witchcraft, voodoo or the occult?
Some of these delusions are relatively commonly held beliefs that can cause high levels of distress, make life difficult to live and socially isolate you from others that don’t share your belief, all while not having schizophrenia.
For example delusional jealousy, is an all too common phenomena. We all know someone has let their social media stalking green-eyed monster rear their ugly head, despite having no proof or justifiable reason to believe anything untoward is going on. Likewise, delusions of reference are pretty standard day to day operations for many healthy individuals, where a person falsely believes that insignificant remarks, events, or objects in one’s environment have personal meaning or significance:
“the clock read 3:33 today, the 33 bus broke down right in front of me and then I was handed 33 cents change. Doo do doo do doo do doo do – the universe is trying to tell me something!”
So ultimately, no matter how bizarre a belief might seem to some, no matter how distressing and life-shattering, it seems that ultimately it is the cultural context which dictates whether a belief is truly delusional or not.
Can delusions be good for us?
On a final note, there is actually evidence suggesting that a certain amount of delusional thinking might actually be good for us! Often we cling onto delusions that make us feel good, or prevent us from feeling bad, whether they are about ourselves, other people or any aspect of life.
For example students may choose to believe more job offers and higher salaries upon graduation are in store for them despite statistics saying otherwise, aiding motivation to complete their studies. Take marriage as another example. Although researchers estimate that 40–50% of all first marriages end in divorce, we marry anyway, many believing unshakably of being together until death do us part, which presumably enhances our feelings of security in the relationship and validates the purpose of the commitment.
Moreover, self-delusional overconfidence in ones abilities and importance, i.e. believing you are better than you are in reality, has been outlined as advantageous in numerous studies as:
“…it serves to increase ambition, morale, resolve, persistence or the credibility of bluffing, generating a self-fulfilling prophecy in which exaggerated confidence actually increases the probability of success.”
In light of this, delusions are not always cognitive flaws, or indeed indicative of schizophrenia and related disorders. They can be life, emotion and peace disrupting; be purposeful and useful features of cognition; or simply be culturally acceptable quirks in our collective thinking and belief system.
Have you ever heard, seen, smelt, felt or tasted something that wasn’t actually there? If you have, you are probably like the overwhelming majority of the world’s population, schizophrenia and psychosis free. Hallucinations, despite common misconceptions, are a part of normal healthy living that most of us put down to a “brain glitch”. Let’s take a look at just how common hallucinating is and how this relates to individuals experiencing schizophrenic hallucinations.
May the destigmitazation commence!
Hallucinations are defined as the perception of an object or event, using any of the five senses (sight, hearing, touch, smell and taste), despite there being no external stimulus. We will leave out hypnagogic (falling asleep) and hypnopompic (waking up) hallucinations, or there we would be no discussion, we would end the debate here by simply stating that we all have the potential to hallucinate practically every day!
For that matter, let’s put sleep deprivation to one side too, as 8 out of 10 of us are likely to have visual hallucinations if sleep deprived for long enough. The longer you go without sleep, the more intense the hallucination. Moreover, forget including childhood in the equation, or bouts of delirious fever.
We should also recognize that even in science research, self-reports of hallucinations are likely under-reported in healthy people for multiple reasons. One reason established by research is an individuals fear of appearing insane. Thankfully, reports of hallucinations are not so easily effected by the need to be socially desirable as reports of delusions are.
A revealing analysis of the World Health Organization’s World Health Survey from 52 countries indicates that the frequency of self-reports of hallucinations in the general population are greatly impacted by culture. For example, estimates of the number of people reporting hallucinations over a 12 month period in Nepal were a hearty 32%. Meanwhile, in Kazakhstan this number was a meagre 0.5%.
While currently there aren’t any real, solid ideas as to why, and more questions being posed than answers being given, let’s put cultural differences aside and take a look at the various forms of hallucinations in a little more detail.
Auditory Hallucinations
“What? Did someone call my name?”
Auditory hallucinations are the most commonly reported type of hallucination in schizophrenia (present in 60-90% of patients) and most commonly manifests as hearing voices, with music hearing also being commonly reported.
One of the largest and most detailed studies on hearing voices estimates that 5-15% of all adults will experience hearing voices at some point during their lifetimes. One percent of these healthy, non-schizophrenic individuals may hear multiple and at times interacting voices with character-like qualities that are typically associated with chronic schizophrenic hallucinations. For many, it’s just a normal mode of experience.
Visual Hallucinations
“I am sure there was a man standing there!”
Visual hallucinations typically involve flashes of light or sightings of people and/or animals and are the second most commonly reported type of hallucination in schizophrenia (16-72% of patients). Let’s not forget that in certain religious circles, seeing a flash of light may be considered a gift or glimpse of God.
Reports estimate that 4-12% of healthy individuals have visual hallucinations (although numbers vary greatly between different countries, as mentioned previously).
Tactile and Somatic Hallucinations
“Ahhhh! Was that a beasty crawling up my leg?!”
Tactile hallucinations involve sensations felt on the skin, like being tapped on the shoulder or an insect crawling along the surface. Somatic hallucinations on the other hand involve more internal physical sensations, like feelings of electricity in the brain or snakes slithering inside the stomach.
One US-based study estimates that tactile and somatic hallucinations occur in around 20% of schizophrenic patients. Currently, how common this is in the general populace is largely unknown. One UK report estimates that 3% of the population experience touch-based hallucinations, 24% of which have no association with poor mental health.
Olfactory and Gustatory Hallucinations
“Can you smell/taste that? No? Just me?”
Olfactory (smell) and gustatory (taste) hallucinations, known as phantosmia and gustatory phantasma respectively, are the least reported hallucinations in schizophrenic patients. This may very well be because they are less distressing and less infamous, but that does not necessarily mean that they are uncommon, and are suspected to be grossly under-reported.
In a US-based study, 17% and 8% of schizophrenic patients experienced olfactory and gustatory hallucinations respectively. Interestingly, initial estimates of hallucinations of smell and taste in the general UK population are pretty similar at 7-8%, with 2-3% of participants having had experienced the hallucinations the month prior to when the study was conducted.
Hallucinations in Schizophrenia
So what is the difference between hallucinations experienced when a person is diagnosed as schizophrenic, compared to when they are diagnosed as mentally healthy? Its worthy of note that not all schizophrenic patients experience hallucinations, with the International Pilot Study of Schizophrenia estimating that approximately 70% of schizophrenic patients experience them. For those that do they are rarely benign or pleasant.
In the schizophrenic population, these hallucinations – that healthy people tend to chalk down to an intriguing blip in reality – are more frequent, intrusive and distressing. The real game-changer is when one believes that these glitches in our naturally skewed, flawed and limited interpretation of reality are real.
Hallucinations as a Sign of Ill-Health?
That being said, there are numerous reports of hallucinations being associated with physical health problems independently of a mental disorder, and those that persist may be worthy of clinical examination. They are often reported in individuals with epilepsy, brain tumors, migraines, visual impairment, stroke, drug withdrawal, sinus diseases, sensory deprivation, narcolepsy, inborn errors of metabolism and various neurodegenerative diseases.
However, an individual that is blessed by never having mental health issues and is in perfect physical health may still experience regular hallucinations. Experiencing hallucinations are far more common than schizophrenia or a related mental disorder, as well as most of the more physical ailments that hallucinations are associated with!
With the misplaced idea that hallucinating is a dead cert sign of mental illness free from your mind, please feel free to share your hallucinatory experiences and let’s see just how common they are.
From:
http://brainblogger.com/2015/04/10/are-we-all-schizophrenic-part-1-delusions/
References
Armando M, Nelson B, Yung AR, Ross M, Birchwood M, Girardi P, & Fiori Nastro P (2010). Psychotic-like experiences and correlation with distress and depressive symptoms in a community sample of adolescents and young adults. Schizophrenia research, 119 (1-3), 258-65 PMID: 20347272
Freeman D (2006). Delusions in the nonclinical population. Current psychiatry reports, 8 (3), 191-204 PMID: 19817069
Hatzenbuehler ML, Phelan JC, & Link BG (2013). Stigma as a fundamental cause of population health inequalities. American journal of public health, 103 (5), 813-21 PMID: 23488505
Johnson DD, & Fowler JH (2011). The evolution of overconfidence. Nature, 477 (7364), 317-20 PMID:21921915
Knowles R, McCarthy-Jones S, & Rowse G (2011). Grandiose delusions: a review and theoretical integration of cognitive and affective perspectives. Clinical psychology review, 31 (4), 684-96 PMID:21482326
Lincoln TM, & Keller E (2008). Delusions and hallucinations in students compared to the general population. Psychology and psychotherapy, 81 (Pt 3), 231-5 PMID: 18426692
Peters ER, Joseph SA, & Garety PA (1999). Measurement of delusional ideation in the normal population: introducing the PDI (Peters et al. Delusions Inventory). Schizophrenia bulletin, 25 (3), 553-76 PMID: 10478789
Peters E, Joseph S, Day S, & Garety P (2004). Measuring delusional ideation: the 21-item Peters et al. Delusions Inventory (PDI). Schizophrenia bulletin, 30 (4), 1005-22 PMID: 15954204
Beavan V, Read J, & Cartwright C (2011). The prevalence of voice-hearers in the general population: a literature review. Journal of mental health (Abingdon, England), 20 (3), 281-92 PMID: 21574793
Chabrol H, Chouicha K, Montovany A, & Callahan S (2001). [Symptoms of DSM IV borderline personality disorder in a nonclinical population of adolescents: study of a series of 35 patients].L’Encephale, 27 (2), 120-7 PMID: 11407263
DeVylder JE, & Hilimire MR (2014). Screening for psychotic experiences: social desirability biases in a non-clinical sample. Early intervention in psychiatry PMID: 24958508
Kessler, R., Birnbaum, H., Demler, O., Falloon, I., Gagnon, E., Guyer, M., Howes, M., Kendler, K., Shi, L., Walters, E., & Wu, E. (2005). The Prevalence and Correlates of Nonaffective Psychosis in the National Comorbidity Survey Replication (NCS-R) Biological Psychiatry, 58 (8), 668-676 DOI:10.1016/j.biopsych.2005.04.034
Lewandowski KE, DePaola J, Camsari GB, Cohen BM, & Ongür D (2009). Tactile, olfactory, and gustatory hallucinations in psychotic disorders: a descriptive study. Annals of the Academy of Medicine, Singapore, 38 (5), 383-5 PMID: 19521636
Moreno C, Nuevo R, Chatterji S, Verdes E, Arango C, & Ayuso-Mateos JL (2013). Psychotic symptoms are associated with physical health problems independently of a mental disorder diagnosis: results from the WHO World Health Survey. World psychiatry : official journal of the World Psychiatric Association (WPA), 12 (3), 251-7 PMID: 24096791
Ohayon MM (2000). Prevalence of hallucinations and their pathological associations in the general population. Psychiatry research, 97 (2-3), 153-64 PMID: 11166087
Teeple, R., Caplan, J., & Stern, T. (2009). Visual Hallucinations The Primary Care Companion to The Journal of Clinical Psychiatry, 11 (1), 26-32 DOI: 10.4088/PCC.08r00673