Buvidal : a new hope for opiate addiction?
What is Opioid Agonist Treatment (OAT)?
- OAT (previously called OST) is an effective treatment for heroin and other opioid addiction. The longer you stay on OAT, the more likely you are to stop using opioids.
- In NSW Correctional Centres, the injectable Buprenorphine (Buvidal) is the preferred treatment for managing addiction to opioids.
- Anyone entering custody on OAT continues on treatment (unless there is a medical or health reason why they should not). If you were on Suboxone in the community, you will be moved to Buvidal.
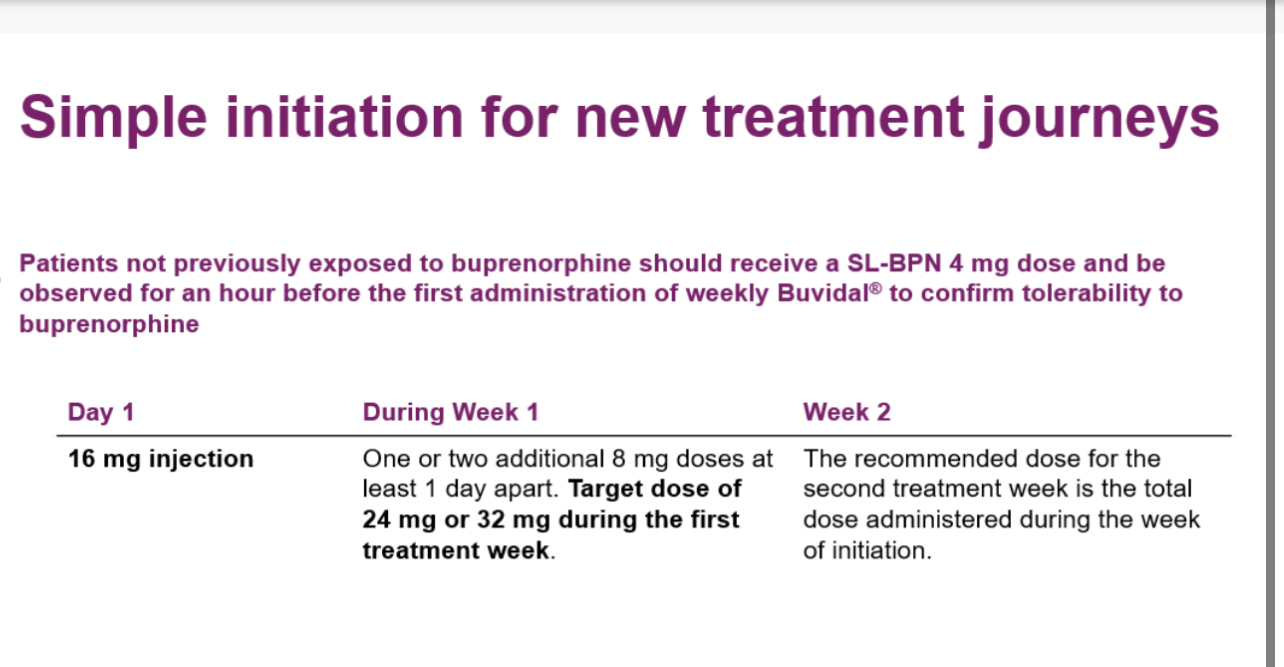
Here’s a general medical protocol for using Buvidal (long-acting buprenorphine) in a day case hospitalization setting for an opioid-dependent patient. Please note that this should be adapted based on specific institutional guidelines and individual patient needs.
Suggested Protocol for Buvidal (long-acting buprenorphine) Initiation in Day Case Setting:
- Pre-admission Assessment:
- Confirm opioid dependence diagnosis
- Review medical history and current medications
- Assess for contraindications to buprenorphine
- Perform baseline liver function tests
- Obtain informed consent
- Admission Day: a. Initial Assessment:
- Verify last opioid use (time and amount)
- Assess withdrawal symptoms using COWS (Clinical Opiate Withdrawal Scale)
- Perform urine drug screen
- Check vital signs
- If COWS < 12: Continue monitoring until moderate withdrawal
- If COWS 12-16: Proceed with Buvidal administration
- If COWS > 16: Provide symptomatic relief and reassess
- Determine appropriate dose based on opioid tolerance:
- 64 mg or 96 mg for moderate to high opioid tolerance
- 32 mg for lower tolerance or transitioning from low-dose opioids
- Administer Buvidal subcutaneously in the abdominal area
- Record time of administration and dose given
- Monitor vital signs every 30 minutes for 2 hours
- Assess for signs of precipitated withdrawal or adverse reactions
- Provide symptomatic relief if needed (e.g., anti-emetics, NSAIDs)
- Explain expected effects and potential side effects
- Provide information on follow-up appointments and emergency contacts
- Discuss the importance of abstinence from other opioids
- Stable vital signs
- No signs of severe withdrawal or adverse reactions
- Patient alert and oriented
- Arrangement for safe transportation home
- Follow-up Plan:
- Schedule next Buvidal dose (weekly or monthly as appropriate)
- Arrange for outpatient follow-up within 1 week
- Provide prescriptions for any necessary adjunct medications
- Documentation:
- Complete all necessary medical records
- Provide discharge summary to the patient and their primary care provider
- Emergency Preparedness:
- Ensure naloxone is available during the procedure
- Have protocols in place for managing severe adverse reactions
This protocol provides a framework for Buvidal initiation in a day case setting. It’s crucial to have experienced healthcare providers overseeing the process and to be prepared to adapt the protocol based on individual patient responses.
Exact timing when to start:
The timing for starting Buvidal (long-acting buprenorphine) in a morphine-dependent patient is crucial to minimize withdrawal symptoms and ensure a smooth transition. Here’s a general guideline:
- Assess the patient’s last morphine use:
- Timing depends on when the patient last used morphine and their level of physical dependence.
- Wait for mild to moderate withdrawal:
- Ideally, start Buvidal when the patient is experiencing mild to moderate withdrawal symptoms.
- This usually occurs 12-24 hours after the last morphine use, depending on the dosage and frequency.
- Use objective withdrawal scales:
- Employ scales like the Clinical Opiate Withdrawal Scale (COWS) to assess withdrawal severity.
- A COWS score of 12-16 (moderate withdrawal) is often considered appropriate for initiation.
- Consider the half-life of morphine:
- Morphine’s half-life is relatively short (2-3 hours), so withdrawal symptoms may appear sooner compared to longer-acting opioids.
- Avoid precipitated withdrawal:
- Starting too early can cause precipitated withdrawal, which is more severe and sudden.
- Individual factors:
- Consider the patient’s overall health, other medications, and specific circumstances.
- Supervised initiation:
- The first dose should be given under medical supervision to monitor for adverse reactions.
- Dosing considerations:
- The initial dose of Buvidal will depend on the patient’s level of opioid tolerance.
- Transition period:
- Some clinicians may use short-acting buprenorphine first before transitioning to Buvidal.
- Patient education:
- Inform the patient about what to expect and the importance of timing.
- For Patients taking methadone :
- Methadone dose should be reduced to 30 mg/ day and wait 24 hours before starting (Buvidal).
- For Heroin or short acting Opioids:
- should wait 6 hours before starting (Buvidal).
It’s critical to note that these are general guidelines. The exact timing and protocol should be determined by the healthcare provider experienced in addiction medicine, working in the place, taking into account the individual patient’s specific situation and needs.


