CVS and Psychiatric Presentation
Could a routine MRI scan reveal hidden risks for stroke, dementia, and severe depression? White matter hyperintensities (WMHs) are more than just age-related changes—they may serve as critical markers for neuropsychiatric disease progression.
Research consistently links WMHs to serious neuropsychiatric outcomes:
- A meta-analysis in BMJ found that WMHs significantly increase the risk of stroke, dementia, and cognitive decline, even after controlling for vascular risk factors.
- Studies suggest a strong association with late-onset and treatment-resistant depression, particularly in patients with psychomotor slowing and executive dysfunction.
- In some cases, WMH burden has been shown to progress within 12 weeks, correlating with worsening mood and cognitive symptoms.
What Does This Mean for Psychiatric Practice?
WMHs may be a crucial biomarker for identifying high-risk patients early, tailoring treatment strategies, and preventing long-term neurological decline. By integrating neuroimaging insights into psychiatric assessments, clinicians can improve diagnostic accuracy and optimise long-term outcomes.

49 year old female presenting with resistant depression and mixed features. Frontal lobe testing showed executive dysfunction. Required augmentation strategies to achieve remission
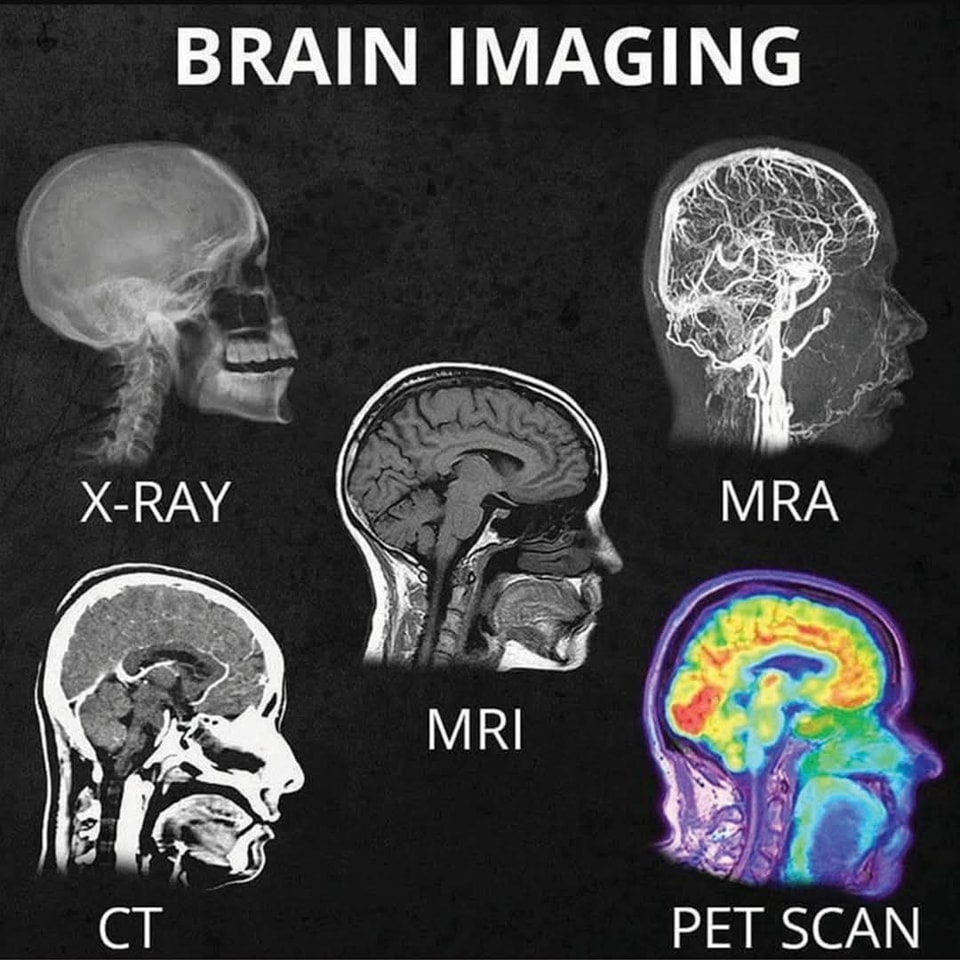
Given the increasing clinical relevance of white matter hyperintensities, understanding neuroimaging techniques is becoming essential for psychiatrists. Recognizing these findings early can significantly impact diagnosis and treatment strategies.
Brain Stroke and Psychiatric Presentation
Introduction
- A brain stroke (cerebrovascular accident) occurs when blood flow to part of the brain is interrupted, leading to brain cell damage.
- Strokes can have significant psychiatric consequences, both in the acute phase and as long-term sequelae.
- Psychiatric symptoms may arise from the location of the stroke, the psychological impact of the event, or underlying risk factors.
Types of Stroke
- Ischemic Stroke:
- Caused by a blockage in a blood vessel (e.g., clot).
- Accounts for ~85% of strokes.
- Hemorrhagic Stroke:
- Caused by bleeding in or around the brain (e.g., ruptured aneurysm).
- Accounts for ~15% of strokes.
Psychiatric Presentations of Stroke
- Post-Stroke Depression (PSD):
- Prevalence: Occurs in ~30% of stroke survivors.
- Symptoms:
- Persistent sadness, hopelessness, or anhedonia.
- Fatigue, sleep disturbances, and appetite changes.
- Mechanism:
- Disruption of monoamine pathways (e.g., serotonin, norepinephrine).
- Lesions in the left frontal lobe are particularly associated with depression.
- Treatment:
- Antidepressants (e.g., SSRIs like sertraline).
- Psychotherapy (e.g., cognitive-behavioral therapy).
- Post-Stroke Anxiety:
- Prevalence: Occurs in ~20–25% of stroke survivors.
- Symptoms:
- Excessive worry, restlessness, or panic attacks.
- Fear of recurrent stroke.
- Mechanism:
- Dysregulation of the limbic system and amygdala.
- Treatment:
- SSRIs or benzodiazepines (short-term).
- Relaxation techniques and psychotherapy.
- Post-Stroke Psychosis:
- Prevalence: Rare (~1–2% of stroke survivors).
- Symptoms:
- Hallucinations (often visual or auditory).
- Delusions (e.g., paranoia).
- Mechanism:
- Lesions in the right hemisphere or thalamus.
- Treatment:
- Antipsychotics (e.g., quetiapine, risperidone).
- Post-Stroke Emotional Lability (Pseudobulbar Affect):
- Prevalence: Occurs in ~10–20% of stroke survivors.
- Symptoms:
- Uncontrollable laughing or crying unrelated to mood.
- Mechanism:
- Disruption of corticobulbar pathways.
- Treatment:
- Dextromethorphan/quinidine (Nuedexta).
- SSRIs or tricyclic antidepressants.
- Post-Stroke Cognitive Impairment:
- Prevalence: Occurs in ~30–50% of stroke survivors.
- Symptoms:
- Memory deficits, attention problems, and executive dysfunction.
- May progress to vascular dementia.
- Mechanism:
- Damage to cortical or subcortical regions involved in cognition.
- Treatment:
- Cognitive rehabilitation.
- Cholinesterase inhibitors (e.g., donepezil) for dementia.
- Post-Stroke Apathy:
- Prevalence: Occurs in ~20–40% of stroke survivors.
- Symptoms:
- Lack of motivation, interest, or emotional responsiveness.
- Mechanism:
- Lesions in the frontal lobes or basal ganglia.
- Treatment:
- Stimulants (e.g., methylphenidate) or dopamine agonists.
- Behavioral activation therapy.
Risk Factors for Psychiatric Complications
- Stroke Location:
- Left frontal lobe: Depression.
- Right hemisphere: Psychosis or emotional lability.
- Thalamus or basal ganglia: Cognitive or mood disturbances.
- Severity of Stroke:
- More severe strokes are associated with higher rates of psychiatric sequelae.
- Premorbid Psychiatric History:
- Patients with a history of depression or anxiety are at higher risk.
- Social and Environmental Factors:
- Lack of social support or financial stress can exacerbate symptoms.
Management of Psychiatric Symptoms Post-Stroke
- Early Screening:
- Use validated tools (e.g., PHQ-9 for depression, GAD-7 for anxiety).
- Multidisciplinary Approach:
- Collaborate with neurologists, psychiatrists, and rehabilitation specialists.
- Pharmacological Treatment:
- SSRIs for depression and anxiety.
- Antipsychotics for psychosis.
- Nuedexta for emotional lability.
- Non-Pharmacological Interventions:
- Cognitive-behavioral therapy (CBT).
- Cognitive rehabilitation for memory and executive function.
- Support groups for stroke survivors.
Key Takeaways
- Strokes can lead to a wide range of psychiatric symptoms, including depression, anxiety, psychosis, emotional lability, and cognitive impairment.
- The location and severity of the stroke play a key role in determining the psychiatric presentation.
- Early recognition and treatment are essential to improve quality of life and functional outcomes.

