Normal Pressure Hydrocephalus:
Etiology and Course of illness :
What causes normal pressure hydrocephalus?
NPH occurs if the normal flow of CSF throughout the brain and spinal cord is blocked in some way. This may be due to past injury, bleeding, infection, brain tumor, or surgery on the brain, or the cause is often not known. When excess CSF fluid builds up in the ventricles, they enlarge and press against nearby brain tissue. This extra fluid and pressure can lead to brain damage.
NPH is rare. It most often affects older adults, and its symptoms can be like those of Alzheimer and Parkinson diseases. A healthcare provider familiar with these conditions can often tell the difference between these diseases and NPH after special testing.
Normal pressure hydrocephalus (NPH) is a condition characterized by the buildup of cerebrospinal fluid (CSF) in the brain ventricles, leading to a range of symptoms.
The course of illness for NPH typically progresses in stages, with varying degrees of severity.
Initial Symptoms
The initial symptoms of NPH often begin gradually and may include:
- Gait disturbances: Patients may experience difficulty walking, stumbling, or feeling unsteady.
- Urinary urgency and/or incontinence: Patients may experience a sudden and intense need to urinate, leading to incontinence.
- Cognitive deficits: Patients may experience memory loss, confusion, or difficulty with complex tasks.
Progression of Symptoms
As the condition progresses, symptoms may worsen and new ones may emerge. The typical progression of symptoms includes:
- Gait disturbances: Patients may experience increased difficulty walking, stumbling, or feeling unsteady, which can lead to falls.
- Urinary incontinence: Patients may experience more frequent or severe episodes of incontinence.
- Cognitive deficits: Patients may experience increased memory loss, confusion, or difficulty with complex tasks, which can impact daily life.
- Dementia: Patients may experience a decline in cognitive function, leading to difficulty with daily activities, communication, and problem-solving. The patient might be insightful for the situation and has a sense of poor ability for word finding and phrase expression so either goes for catastrophic reaction (anger burst irrational) or resign from surroundings and resorts to withdrawal.
Complications
Untreated or poorly managed NPH can lead to complications, including:
- Falls: Patients may experience increased risk of falls due to gait disturbances. This symptom could be the first presentation and the starting noticeable unexplained symptom.
- Urinary tract infections: Patients may experience increased risk of urinary tract infections due to incontinence.
- Depression:
- Patients may experience depression due to the impact of NPH on daily life and cognitive function. The case can be presented for the first time to a psychiatrist without past history of depression. Depressed mood is attributed to poor cognitive ability to word finding, focus, catastrophic reaction, inability to self care, sense of being burden on others, helpless regarding incontinence of urine even when mild
- Caregiver burden:
- Caregivers may experience emotional and physical strain due to the demands of caring for a patient with NPH.
Treatment and Management
Treatment and management of NPH typically involve a combination of medication, physical therapy, and surgery. The goal of treatment is to reduce symptoms, improve quality of life, and slow the progression of the condition.
Practice Essentials
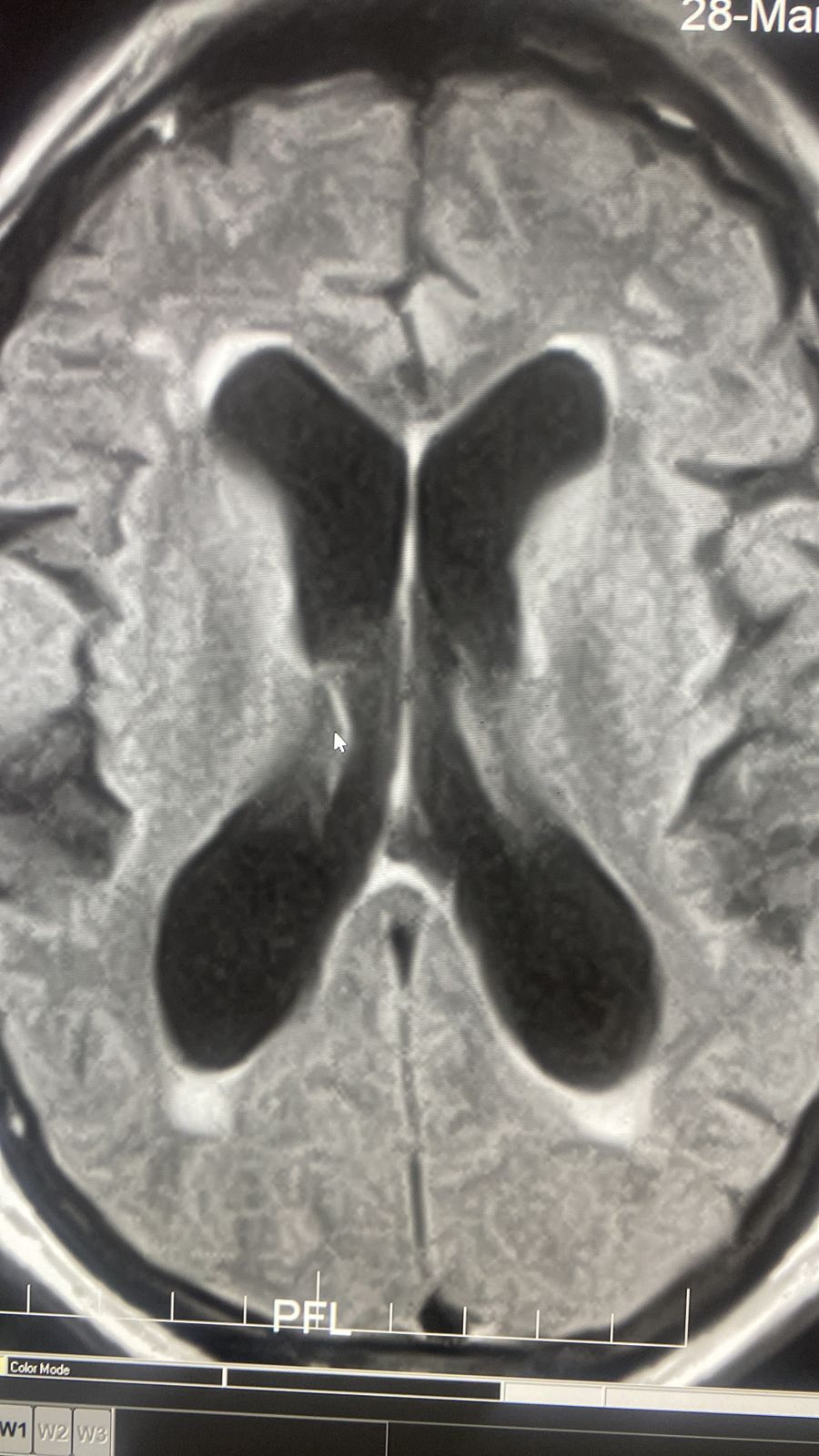
Normal pressure hydrocephalus (NPH) is a clinical symptom complex caused by the build-up of cerebrospinal fluid. This condition is characterized by abnormal gait, urinary incontinence, and (potentially reversible) dementia. See the image below.
Signs and symptoms
Patients with NPH present with a gradually progressive disorder. The classic triad consists of the following:
- Abnormal gait: Earliest feature and most responsive to treatment; bradykinetic, broad-based, magnetic, and shuffling gait
- Urinary incontinence: Urinary frequency, urgency, or frank incontinence
- Dementia: Prominent memory loss and bradyphrenia; forgetfulness, decreased attention, inertia

Diagnosis
Laboratory testing
In general, laboratory testing is not helpful in the diagnosis of NPH. However, a levodopa challenge may be helpful to rule out idiopathic Parkinson disease; patients with NPH have no significant response to levodopa or dopamine agonists.
Imaging studies
Imaging studies are invaluable in the diagnosis of NPH. In most cases of new-onset neurologic symptoms, obtain an initial computed tomography scan of the brain. Although magnetic resonance imaging is more specific than CT scanning in NPH, a normal CT scan can exclude the diagnosis.

Procedures
All patients with suspected NPH should undergo diagnostic CSF removal (either large volume lumbar puncture and/or external lumbar drainage), which has both diagnostic and prognostic value. Improvement in symptoms with large-volume drainage supports the diagnosis of NPH.
Management: Surgery

Surgical CSF shunting remains the main treatment modality for NPH. Prior to embarking upon surgical therapy, knowing which patients may benefit from surgery is necessary. Detailed testing is performed before and after CSF drainage (eg, baseline neuropsychological evaluation, timed walking test, large-volume lumbar puncture, external lumbar drainage, CSF infusion testing).
Ideal candidates for shunt surgery would show imaging evidence of ventriculomegaly, as indicated by a frontal horn ratio exceeding 0.50 on imaging studies, along with one or more of the following criteria:
- Presence of a clearly identified etiology
- Predominant gait difficulties with mild or absent cognitive impairment
- Substantial improvement after CSF withdrawal (CSF tap test or lumbar drainage)
- Normal-sized or occluded sylvian fissures and cortical sulci on CT scan or MRI
- Absent or moderate white-matter lesions on MRI
An alternative technique to shunt surgery is endoscopic third ventriculostomy.
Pharmacotherapy
No definitive evidence exists that medication, including levodopa/carbidopa, can successfully treat NPH. Although levodopa/carbidopa has been reported to be of benefit in anecdotal reports, patients with NPH may represent misdiagnosed cases of parkinsonism. However, in patients who are poor candidates for shunt surgery, repeated lumbar punctures in combination with acetazolamide may be considered.
Lumbar Drain Trial
A drain trial is a “test drive” to determine if a CSF shunt will improve the patient’s symptoms. If the patient is taking blood-thinners, he or she is required to stop the medication 7 to 10 days prior to the trial. The patient then is admitted to the hospital. Upon admission, a physical therapist evaluates the patient’s gait to establish a baseline of their balance and stride.
In a lumbar drain, a hollow needle is inserted into the fluid-filled subarachnoid space in the lower spine. A flexible catheter is inserted through the hollow needle and the needle is removed.
Cerebrospinal fluid (CSF) is collected for a few days and CSF pressure is monitored.
A local anesthetic is used to numb the area in the lower back. The surgeon inserts a temporary catheter into the spinal canal to drain CSF (Fig. 4). The patient remains in the hospital for 3 to 4 days while CSF is drained periodically and your condition is monitored, especially your walking ability. Family and friends may visit and keep you company.
After 72 hours, the drain is removed and the physical therapist performs a second evaluation of the patient’s gait. A repeat neuropsychological exam is also performed. If the patient’s memory and gait are markedly improved following the drain trial, a positive diagnosis of NPH can be made.
Any improvement in symptoms from the drain trial will last only a few days. Symptoms will return to their previous state.
If, after testing, physicians determine that a patient does not have NPH, the patient should be referred to a neurologist. The neurologist will consider whether the patient has another disease that mimics NPH, such as Alzheimer’s disease or brain atrophy. Treatment will depend on the actual disease process that is occurring.
What treatments are available?
There is no cure for NPH, and there is no medication available. However, a CSF shunt can provide symptom relief to some patients. Implanted surgically, the device removes excess fluid from the ventricles. If the lumbar drain trial is successful, the patient may be a good candidate for a permanent CSF shunt. Because NPH is usually a progressive disorder, the shunt extends quality of life for the patient but symptoms of NPH may return.
Sometimes a patient with NPH may be unable to have a shunt because of other health problems that would make surgery unsafe. Treatment of that condition may improve the patient’s health enough so that he or she can undergo shunt surgery safely.
Shunt surgery
A neurosurgeon and general surgeon work together to implant a ventricular peritoneal (VP) shunt.
The flexible, tube-like device drains excess CSF from the brain to the belly area

A programmable shunt has three parts:
(1) a ventricular catheter that connects to a
(2) valve system that regulates the pressure or flow of CSF down a
(3) peritoneal catheter into the abdominal space.
The shunt has a valve that opens to release fluid when the pressure builds up. The fluid drains into the abdominal space and is later absorbed. The drain tube can also be placed into the lung or the jugular vein. The surgery is performed under general anesthesia and lasts about 90 minutes.
Step 1. An incision is made in the scalp at the back of the head. A small hole is drilled in the skull. A catheter is passed through the brain to rest inside the enlarged ventricle.
Step 2. An incision is made behind the ear. The shunt/valve is inserted and the ventricular catheter is attached.
Step 3. Another incision is made in the belly. Next, a tunnel is created under the skin from behind the ear, extending down the neck and chest and into the abdominal area. A peritoneal catheter is connected to the shunt/valve to carry the excess CSF to the belly, where it will be absorbed.
What happens after surgery?
The patient remains in the hospital 2 to 3 days.
At first, the area over the shunt may be raised up, but as the swelling goes away, the shunt is usually not noticeable. Spinal headaches are caused by leakage of CSF around the catheter or shunt site.
Lie flat and drink plenty of caffeinated noncarbonated fluids (e.g., tea, coffee).
Patients should take it easy for several weeks after surgery, with no bending, twisting, heavy lifting, or wearing of tight-fitting hats. Incisions need time to heal. Patients may shower as directed by their surgeon but should not take a tub bath or submerge in water for 4 weeks.
Incisions should be patted dry with a soft towel to avoid irritation.
If the patient has a severe headache, vomiting, and a stiff neck that prevents lowering the chin to the chest — this is an emergency — go to a hospital. These are signs of bleeding in the brain.
Recovery
Most patients with an NPH shunt will see the neurosurgeon 2 to 3 times during the first year following their surgery. The first visit occurs shortly after surgery and involves checking the incision and following up with any issues the patient might be having during the early recovery period.
Later follow-up visits will involve an evaluation to make sure the shunt isn’t draining too much or too little. If necessary, the doctor can adjust the shunt programming with a controller from outside the body without additional surgery. The physician may also request a CT scan to check the ventricles.
In some cases, a non-programmable shunt will be implanted. Placement of an adjustable vs. non- adjustable shunt valve is a matter of preference and debate among neurosurgeons. Talk to your doctor about which device is best for your situation.
What are the risks?
No surgery is without risk. Potential complications from the surgery itself include bleeding in the brain or ventricles, infection, seizures, and problems with anesthesia.
Complications that can occur later include shunt malfunction from a clog or infection. This causes CSF to build up and a return of the original symptoms. Call the doctor if you experience abnormal symptoms. Blockages can often be fixed. In rare cases, the shunt may need to be replaced.
If the ventricles decrease in size too rapidly, the brain can pull away from the skull and tear small blood vessels. This can cause blood clots around brain (called a subdural hematoma). Programming of the shunt to drain CSF at the proper rate and regular follow up visits with the doctor ensures the system is working optimally.
Some symptoms of shunt malfunction:
- Difficulty walking/gait disturbances
- Cognitive problems/mild dementia
- Urinary urgency or incontinence
- Fever (sign of shunt failure or infection)
- Redness along the shunt tract (sign of shunt failure or infection)
What are the results?
Some patients treated with a shunt will have dramatic symptom relief. Studies show that 50 to 80% of patients can expect improvement of their symptoms in the first 2 to 3 years [1].
Other patients may have a less successful outcome. Several factors determine the outcome, including the patient’s overall health, what caused the NPH to occur, and how long the patient has had NPH.
Early diagnosis and treatment improve the odds of having successful symptom relief with a shunt. Patients who have had symptoms for less than a year or have mild to no dementia do better [2].
Men, and all patients of advanced age, are less likely to show improvement in thinking and memory after a shunt operation [3].
Another study found that while significant improvement in ataxic gait and urinary incontinence can occur, improvement of dementia is uncommon [4].
Why some patients improve and others do not is the result of two factors. First, scientists do not completely understand what factors cause NPH to occur. Second, neurosurgeons differ on how to diagnose, treat, and measure success in patients with NPH.
Because NPH is a lifelong disease, an implanted shunt can provide relief of symptoms, but it cannot provide a cure.
Sources
Sources
1. Marmarou A, Bergsneider M, Felkin N, et al. Development of guidelines for idiopathic normal-pressure hydrocephalus. Neurosurgery 57 (Suppl):S1-3, 2005
2. Meier U, Konig A, Miethke C. Predictors of outcome in patients with normal-pressure hydrocephalus. Eur Neurol 51:59-67, 2004
3. Chang s, Agarwal S, Williams MA, et al. Demographic factors influence cognitive recovery in idiopathic normal pressure hydrocephalus after shunt. Cogn Behav Neurology 17:179-184, 2004
4. Poca MA, Mataro M, Matarin M, et al. Good outcome in patients with normal-pressure hydrocephalus and factors indicating poor prognosis. J Neurosurg 103:455-463, 2005



