Venlafaxine: unleashed Secrets
The story behind discovery
1993: The immediate-release form of venlafaxine (Effexor®), a serotonin-norepinephrine reuptake inhibitor (SNRI), was approved by the FDA for the treatment of major depressive disorder (MDD) in the United States.
1997:
The extended-release form of venlafaxine was also approved for MDD treatment.
Key Milestones
Introduction of the first “Atypical” antidepressant drug, venlafaxine, targeting serotonin and norepinephrine transporters, in 1993.
Initial dose and maintenance dose guidelines established for extended-release venlafaxine, with a maximum daily dose of 225 mg.


The Discoverer
Dr. Abou-Gharbia has held a number of leadership positions since joining Temple. He served as Pharmacy’s Associate Dean for Research from 2008-2019 and as the director of the Moulder Center for Drug Discovery Researchfrom 2008-2020.
In recognition of his contributions and success he was named Laura H. Carnell Professor in 2013 and Temple University Outstanding Service Award (2022).
Magid’s research has resulted in over 130 publications. He has co-authored 5 book chapters and delivered over 235 presentations as an invited lecturer at scientific conferences and academic institutions worldwide. He holds over 125 issued US patents and over 350 issued world patents. Magid has received numerous awards in recognition for his research contributions including two ACS Heroes of Chemistry awards for discovery of Effexor® and Torisel®, Induction into New Jersey Inventors Hall of Fame and the ACS
Medicinal Chemistry Hall of Fame, Proctor Medal, Chemical Pioneer Award,
Pennsylvania Bio Award and Educator of the Year Award, Grand Hamdan
Award for Excellence in Biomedical Sciences and Drug Discovery.
The Discoverer
the receptor occupancy and venlafaxine drug response relation?
Let me explain the relationship between receptor occupancy and drug response for venlafaxine, which is an important concept in pharmacology.
Venlafaxine Receptor Occupancy vs Clinical Response

Venlafaxine is a serotonin-norepinephrine reuptake inhibitor (SNRI) antidepressant, and its clinical efficacy is closely related to its receptor occupancy. Here’s how the relationship typically works:
- Threshold Effect: A minimum level of receptor occupancy (usually around 50-60%) is required before significant clinical effects are observed.
- Dose-Response Relationship:
- Low occupancy (<30%): Minimal clinical response
- Medium occupancy (30-70%): Increasing clinical response
- High occupancy (>70%): Optimal clinical response
- Plateau Effect: As receptor occupancy approaches 80-90%, the clinical response tends to plateau, meaning additional occupancy doesn’t significantly improve outcomes.
- Sequential Binding:
- At lower doses, venlafaxine primarily occupies serotonin transporters
- As doses increase, norepinephrine reuptake inhibition becomes more prominent
- Clinical Implications:
- Dosing strategies aim to achieve optimal receptor occupancy
- Individual variations in metabolism can affect the relationship
- Side effects may increase with higher receptor occupancy
- Time Course:
- Receptor occupancy occurs relatively quickly
- Clinical response typically lags behind receptor occupancy
- Full therapeutic effect may take several weeks
Understanding this relationship helps in:
- Determining appropriate dosing strategies
- Explaining the delayed onset of action
- Understanding why some patients may need dose adjustments
- Predicting potential side effects at different doses
It’s worth noting that while receptor occupancy is important, other factors also influence clinical response, including:
- Individual patient factors
- Genetic variations
- Concurrent medications
- Overall health status
The graph above illustrates the general relationship between receptor occupancy and clinical response for venlafaxine, showing the typical plateau effect at higher occupancy levels.
The lag between venlafaxine’s receptor occupancy and clinical response is due to several complex neurobiological processes. Let me explain the key factors:
Time Course of Venlafaxine Effects
Let me break down the reasons for this delay:
- Immediate vs. Adaptive Changes
- Immediate effect: Rapid receptor occupancy (within hours)
- Delayed effect: Neuroadaptive changes take weeks
- Key Molecular Mechanisms a) Receptor Downregulation
- Gradual decrease in receptor sensitivity
- Takes days to weeks to fully manifest
- Alterations in intracellular signaling cascades
- Requires time for cellular adaptation
- Genetic Expression Changes
- Activation/suppression of various genes
- Protein synthesis takes time
- New proteins affect neuronal function
- Neuroplasticity
- Synaptogenesis (formation of new synapses)
- Dendritic remodeling
- These structural changes are gradual
- Neurotrophic Factors
- Increased production of BDNF
- Takes time to affect neuronal growth and survival
- Circuit-Level Changes
- Remodeling of neural networks
- Restoration of normal circuit function
- Factors Affecting the Time Course
- Individual genetic variations
- Pre-existing neurobiological state
- Age and metabolic factors
- Concurrent medications
- Clinical Implications
- Patients need to be informed about delayed response
- Early side effects may occur before therapeutic benefit
- Adherence is crucial despite delayed gratification
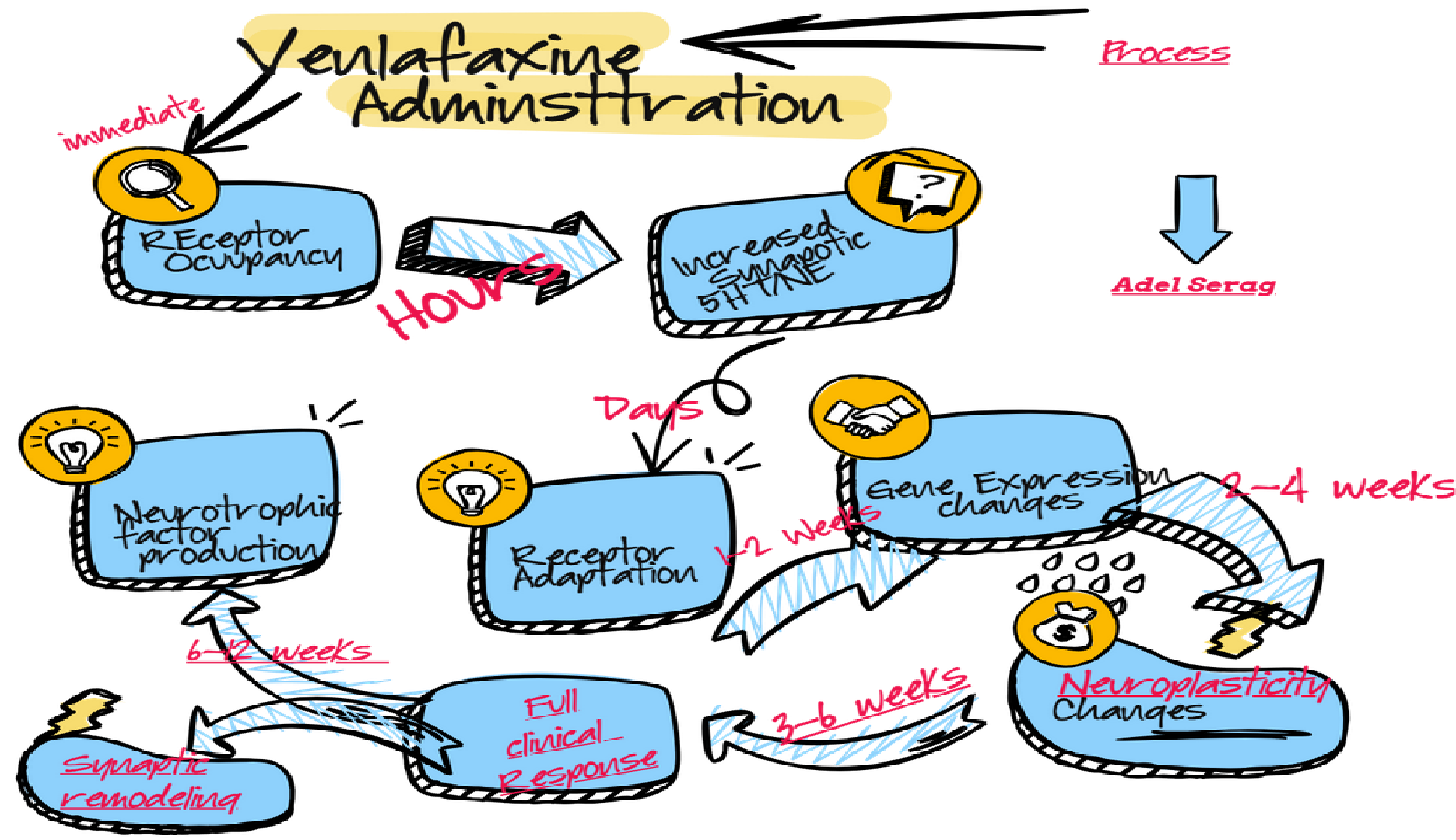
Timing of Events:
- Hours: Receptor occupancy and increased neurotransmitter levels
- Days: Initial receptor adaptations
- 1-2 weeks: Gene expression changes begin
- 2-4 weeks: Neuroplastic changes initiate
- 3-6 weeks: Full clinical response typically observed
The delayed therapeutic response emphasizes the importance of:
- Patient education about expected timeline
- Regular monitoring during the initial weeks
- Maintaining treatment despite lack of immediate improvement
- Understanding that early side effects don’t predict efficacy
Understanding this lag time helps:
- Set appropriate expectations
- Improve treatment adherence
- Guide clinical decision-making
- Inform the development of faster-acting medications
Recent research focuses on:
- Identifying biomarkers of early response
- Developing adjunct treatments to accelerate effects
- Understanding individual factors affecting response time
Based on current pharmacological evidence and clinical practice, alternating high and low daily doses of venlafaxine is generally not recommended for several important reasons:
- Pharmacokinetic Considerations
- Short half-life (5 hours for immediate release)
- Steady-state plasma levels are important
- Alternating doses disrupt steady-state
- Potential Problems with Alternating Dosing
- Inconsistent symptom control
- Increased risk of side effects on high-dose days
- Possible withdrawal symptoms on low-dose days
- Compromised therapeutic efficacy
- Why Consistent Dosing is Preferred
- Maintains stable plasma levels
- Provides consistent receptor occupancy
- Allows for predictable side effect management
- Supports better medication adherence
- Impact on Neurotransmitter Systems
- Serotonin system needs consistent modulation
- Norepinephrine reuptake inhibition varies with dose
- Fluctuating levels may disrupt adaptation
- Clinical Evidence
- Standard practice favors consistent dosing
- No substantial evidence supporting alternating doses
- Clinical trials use consistent daily dosing
- Practical Challenges
- Complicated dosing schedule
- Increased risk of medication errors
- Difficulty tracking therapeutic response
- Special Considerations
- Extended-release formulations designed for steady levels
- Dose adjustments should be gradual when needed
Better Approaches to Dosing:
- Gradual titration to effective dose
- Consistent daily dosing
- Extended-release formulations when appropriate
- Regular monitoring and adjustment as needed
Factors Affecting Dosing Decisions:
- Individual metabolic differences
- Comorbid conditions
- Concurrent medications
- History of response to antidepressants
When Dose Adjustments May Be Needed:
- Inadequate response
- Intolerable side effects
- Changes in other medications
- Development of tolerance
Recommended Strategies:
- Start with lower doses
- Gradually increase to effective dose
- Maintain consistent daily dosing
- Use extended-release formulations when possible
- Regular monitoring of response and side effects
If dose adjustment is needed:
- Make changes gradually
- Monitor closely for effects
- Consider splitting doses if side effects occur
- Aim for the lowest effective dose
Common Dosing Schedules:
- Once-daily dosing (extended-release)
- Twice-daily dosing (immediate-release)
- Consistent dosing at the same time(s) each day
It’s important to note that any changes to medication regimens should be:
- Discussed with a healthcare provider
- Based on individual patient factors
- Monitored closely for effectiveness
- Adjusted based on response and tolerability
Venlafaxine was the first Atypical Noreadrenegic Serotonergic Molecule discovered by Arabic -American Scientist and showed great effecacy in alleviating severe deprssion
Consider dose effect relationship when you do prescribe Venlafaxine and expect permenent changes rather than synaptic receptor response
Consider Nowadays ADHD “Over diagnosis” and consider bipolar disorder in children and teens as well as sof form in adults.
Consider Alternating drug regimen for sleep as well as high to low dose antidepressant and monitor if it is working properly with your patient. Case reports proved it is working

