ﻓﺠﺮ ﻣﻮﻗﻊ ﻣﻐﺮﺑﻲ ﻳﺪﻋﻰ ” ﻣﺎﺭﻭﻙ ﻧﻴﻮﺯ “24 ﻣﻔﺎﺟﺂﺓ ﻗﻮﻳﺔ ﺣﻴﺚ ﻧﺸﺮ ﺻﻮﺭﺓ ﻗﺎﻝ ﺃﻧﻬﺎ ﺗﺜﺒﺖ ﺃﻥ ﺍﻟﺴﻴﺴﻲ ﻛﺎﻥ ﻋﻤﻴﻼ ﻹﺳﺮﺍﺋﻴﻞ ﻭﺃﻧﻬﺎ ﻫﻰ ﻣﻦ ﺟﻨﺪﺗﻪ ﺑﺎﻟﺠﻴﺶ ﺍﻟﻤﺼﺮﻱ .
ﻭﻗﺎﻝ ﺍﻟﻤﻮﻗﻊ : ﻛﻨﺎ ﺳﺎﺑﻘﻮﻥ ﻓﻲ ﺇﻛﺘﺸﺎﻑ ﺃﺻﻞ ﻋﺒﺪ ﺍﻟﻔﺘﺎﺡ ﺍﻟﺴﻴﺴﻲ ﺑﻤﺼﺮ ،ﻭﻧﺸﺮﻧﺎ ﺣﻴﻨﻬﺎ ﺻﻮﺭﺓ ﺃﻣﻪ ﺍﻟﻴﻬﻮﺩﻳﺔ ﺍﻟﻤﻐﺮﺑﻴﺔ ﻭﺍﻟﺘﻲ ﺃﺳﻘﻄﺖ ﻋﻨﻬﺎ ﺍﻟﺠﻨﺴﻴﺔ ﺍﻟﻤﻐﺮﺑﻴﺔ ﻭﺍﻟﺘﻲ ﻛﺎﻧﺖ ﻣﻦ ﺟﺎﺳﻮﺳﺎﺕ ﺍﻟﻜﻴﺎﻥ ﺍﻟﺼﻬﻴﻮﻧﻲ ،ﻭﺍﻟﺘﻰ ﺗﻌﻤﺪﺕ ﺭﺑﻂ ﻋﻼﻗﺎﺕ ﻣﻊ ﻋﻠﻴﺔ ﺍﻟﻘﻮﻡ ﻟﻨﻘﻞ ﺃﺧﺒﺎﺭﻫﻢ ﻭﺇﻏﺘﻴﺎﻟﻬﻢ ﺑﻌﺪ ﺗﺤﺪﻳﺪ ﺃﻣﺎﻛﻨﻬﻢ ، ﺣﻴﻨﻬﺎ ﺍﻟﻜﺜﻴﺮﻳﻦ ﻣﻤﻦ ﻳﻤﻠﻜﻮﻥ ﺍﻷﻓﻖ ﺍﻟﻀﻴﻖ ﺃﺧﺪ ﻳﺴﻌﻰ ﻟﺠﻌﻞ ﺍﻟﺴﻴﺴﻲ ﺑﻄﻼ ﻗﻮﻣﻴﺎ ،ﻓﻴﻤﺎ ﻫﻮ ﻣﺠﺮﺩ ﻋﻤﻴﻞ ﻟﻠﻤﻮﺳﺎﺩ ﺍﻹﺳﺮﺍﺋﻴﻠﻲ ﻭﻗﺪ ﻗﺎﻣﻮﺍ ﺑﺘﺮﺑﻴﺘﻪ ﺗﺮﺑﻴﺔ ﺻﻬﻴﻮﻧﻴﺔ ﺻﺮﻓﻴﺔ ﻋﻠﻰ ﺍﻟﻜﺬﺏ ﻭﺍﻟﺨﺪﺍﻉ ﻭﺟﻌﻠﻮﻩ ﻳﺘﻐﻠﻐﻞ ﺑﺎﻟﺠﻴﺶ ﺍﻟﻤﺼﺮﻱ ﺣﺘﻰ ﻳﻜﻮﻥ ﺍﻟﺴﻴﺴﻲ ﻋﻴﻦ ﺍﻟﻤﻮﺳﺎﺩ ﺩﺍﺧﻠﻪ ،ﻓﻬﻢ ﻳﻌﻠﻤﻮﻥ ﺃﻥ ﺍﻟﺠﻴﺶ ﺍﻟﻤﺼﺮﻱ ﻳﺸﻜﻞ ﺧﻄﺮﺍ ﻋﻠﻴﻬﻢ ﻭﺟﻌﻠﻪ ﻓﻲ ﻗﺒﻀﺘﻬﻢ ﺳﻴﻀﻤﻦ ﻟﻬﻢ ﺩﻭﻟﺔ ﺇﺳﺮﺍﺋﻴﻞ ﺍﻟﻜﺒﺮﻯ ﻣﻦ ﺍﻟﻔﺮﺍﺕ ﻟﻠﻨﻴﻞ .. ﻭﻫﺎﻫﻢ ﺗﻤﻜﻨﻮﺍ ﻣﻦ ﺍﻹﺳﺘﺤﻮﺍﺫ ﻋﻠﻰ ﺍﻟﺠﻴﺶ ﺍﻟﻤﺼﺮﻱ ﺃﻛﺒﺮ ﺟﻴﻮﺵ ﺍﻟﻌﺮﺏ ﻭﺟﻌﻠﻮﻩ ﻓﻲ ﺧﺪﻣﺔ ﺃﺟﻨﺪﺍﺗﻬﻢ ﺍﻟﺼﻬﻴﻮﻧﻴﺔ .
ﻭﺃﺿﺎﻑ ﺍﻟﻤﻮﻗﻊ ﺣﺴﺐ ” ﺍﻟﺘﻘﺮﻳﺮ :” ﻓﻲ ﺻﻮﺭ ﺣﺼﺮﻳﺔ ﻣﺴﺮﺑﺔ ﺗﺒﻴﻦ ﺍﻟﺴﻴﺴﻲ ﺍﻟﻌﻤﻴﻞ ﺣﻴﻨﻤﺎ ﻛﺎﻥ ﻋﻨﺼﺮﺍ ﺑﺎﻟﺠﻴﺶ ﺍﻹﺳﺮﺍﺋﻴﻠﻲ ﻭﻫﻮ ﻳﺘﻠﻘﻰ ﺍﻟﺘﺪﺭﻳﺒﺎﺕ ﻋﻠﻰ ﻳﺪﻳﻪ ،ﻓﺎﻟﺼﻬﺎﻳﻨﺔ ﻭﺗﺨﻄﻴﻄﺎﺗﻬﻢ ﻻ ﺗﺄﺗﻲ ﻭﻟﻴﺪﺓ ﺍﻟﻴﻮﻡ ﺑﻞ ﻫﻲ ﻣﺨﻄﻄﺎﺕ ﻋﻠﻰ ﺍﻷﻣﺪ ﺍﻟﺒﻌﻴﺪ ﻭﺍﻟﺴﻴﺴﻲ ﻛﺎﻥ ﻣﻦ ﺑﻴﻦ ﻣﺨﻄﻄﺎﺗﻬﻢ ﺍﻟﺘﻲ ﺑﻨﻮﻫﺎ ﺣﺠﺮﺓ ﺣﺠﺮﺓ .
ﻓﺤﻴﺎﺓ ﺍﻟﺮﺟﻞ ﺟﺎﺀﺕ ﻏﺎﻣﻀﺔ ﻛﺄﻱ ﺭﺟﻞ ﻣﺨﺎﺑﺮﺍﺕ ﺣﻴﺎﺗﻪ ﻏﺎﻣﻀﺔ ﻧﺸﺄ ﺑﺈﺳﺮﺍﺋﻴﻞ ﻣﻦ ﺃﻡ ﻳﻬﻮﺩﻳﺔ ﺗﺴﻤﻰ ( ﻣﻠﻴﻜﺔ ﺗﻴﺘﺎﺗﻲ ) ﻭﺳﻌﻰ ﻓﻲ ﺑﺪﺍﻳﺎﺗﻪ ﻟﻠﺘﻐﻠﻐﻞ ﺑﺎﻟﺠﻴﺶ ﺍﻟﻤﻐﺮﺑﻲ ﻟﻜﻦ ﻟﻢ ﻳﺘﻤﻜﻦ ﻣﻦ ﺫﻟﻚ ﻟﻴﻘﻀﺔ ﺍﻟﻤﻐﺎﺭﺑﺔ ، ﻓﺘﻢ ﺗﺠﻨﻴﺪﻩ ﻟﻴﺘﻐﻠﻐﻞ ﺑﺎﻟﺠﻴﺶ ﺍﻟﻤﺼﺮﻱ ﺃﻳﺎﻡ ﻣﺒﺎﺭﻙ بالتعاون مع عمر سليمان مدير المخابرات المصرية الذي أشرف على تعيين السيسي شخصيا وتم اغتياله فيما بعد لأنه الوحيد في الجيش المصري الذي يعرف من هو السيسي وتاريخه .
ﺍﻟﺴﻴﺴﻲ ﻓﻲ ﺍﻟﺠﻴﺶ ﺍﻟﺼﻬﻴﻮﻧﻲ
ﻭﻗﺎﻝ ﺍﻟﻤﻮﻗﻊ ﺍﻥ ﻣﺠﺊ ﺍﻟﺴﻴﺴﻲ ﻫﺪﻓﻪ ﺍﻟﻤﻮﺿﻮﻉ ﻣﻦ ﺃﺟﻠﻪ ﻫﻮ ﺍﻹﻋﺪﺍﺩ ﻟﺪﻭﻟﺔ ﺇﺳﺮﺍﺋﻴﻞ ﺍﻟﻜﺒﺮﻯ ﻭﺇﻋﺪﺍﺩ ﺍﻟﺠﻴﺶ ﺍﻟﻤﺼﺮﻱ ﻟﻴﺨﻮﺽ ﺍﻟﺤﺮﺏ نيابة عن الكيان الصهيوني ضد ﺟﻴﻮﺵ ﺷﻤﺎﻝ ﺇﻓﺮﻳﻘﻴﺎ ﻭ من ثم الزﺣﻒ ﻻﺣﺘﻼﻝ ﻣﻜﺔ لأنهم يعتبرونها معقل الإرهاب وان دخول جيش كافر لها يكاد يكون مستحيلا فتم التخطيط ليكون هذا الجيش من جيوش المسلمين ..
ﻓﻬﻞ ﺟﺎﺀ ﻋﻠﻰ ﺍﻟﻌﺮﺏ ﺯﻣﻦ ﻣﻦ ﺍﻟﺪﻫﺮ ﺃﻥ ﺗﻘﻮﺩﻫﻢ ﺇﺳﺮﺍﺋﻴﻞ ﺑﺤﺎﻛﻤﻬﺎ ﻟﻤﺼﺮ ﻋﺒﺪ ﺍﻟﻔﺘﺎﺡ ﺍﻟﺴﻴﺴﻲ ؟؟ ﻓﻤﺎ ﻳﺠﺮﻱ ﺑﻤﺼﺮ ﺇﺫﺍ ﻛﺎﻧﺖ ﺍﻟﺪﻭﻝ ﺍﻟﻌﺮﺑﻴﺔ ﺗﻘﻮﻝ ﺃﻧﻬﺎ ﺑﻌﻴﺪﺓ ﻋﻨﻪ ﻓﻬﻲ ﻭﺍﻫﻤﺔ ﻭﺟﻠﻮﺱ ﺍﻟﺴﻴﺴﻲ ﻋﻤﻴﻞ ﺍﻟﻤﻮﺳﺎﺩ ﻋﻠﻰ ﻋﺮﺵ ﻣﺼﺮ ﻳﻌﻨﻲ ﺍﻟﻘﻀﺎﺀ ﻋﻠﻰ ﺍﻟﻌﺮﺏ ﻭﺍﻹﻋﻼﻥ ﺍﻟﻜﻠﻲ ﻟﺤﺮﺏ ﺑﻨﻲ ﺇﺳﺮﺍﺋﻴﻞ ﻋﻠﻰ ﺍﻟﺪﻳﻦ ﺍﻟﺬﻱ ﺟﺎﺀ ﺑﻪ ﻧﺒﻲ ﺍﻹﺳﻼﻡ ﻣﺤﻤﺪ ﻛﺮﺣﻤﺔ ﻟﻠﻌﺎﻟﻤﻴﻦ …ﻭﺗﺼﺮﻓﺎﺕ ﺍﻟﺴﻴﺴﻲ ﺗﻠﻚ ﺗﺼﺮﻓﺎﺕ ﻛﻠﻬﺎ ﻧﺎﺑﻌﺔ ﻣﻦ ﺗﺮﺑﻴﺘﻪ ﺍﻟﺼﻬﻴﻮﻧﻴﺔ ،ﻋﺪﻡ ﺍﻟﻤﺒﺎﻻﺕ ،ﺍﻟﻨﻔﺎﻕ ﻭﺍﻟﻜﺬﺏ ﻭﺍﻟﻠﻌﺐ ﻓﻲ ﺍﻟﺒﺪﺍﻳﺔ ﻋﻠﻰ ﻭﺗﺮ ﺍﻟﺪﻳﻦ ،ﺃﻱ ﻛﻤﺎ ﻳﻘﺎﻝ ﺑﺎﻟﺪﺍﺭﺟﺔ ( ﻳﺘﻤﺴﻜﻦ ﺣﺘﻰ ﻳﺘﻤﻜﻦ ) .. انظروا إلى الخلبطة في الدين وانظروا للفتاوي الأزهر الأخيرة وانظروا لصلاة العيد المشتركة وانظروا إلى منع الاعتكاف في المساجد في شهر رمضان الماضي وووو و
فقط انتظروا ومن يعش يعرف كثيرا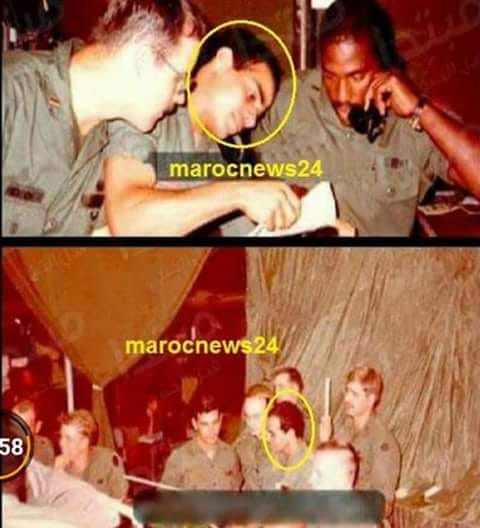
الدواء و الكيمياء
FDA approved psychoactive medication for Children

|
مملكة الجنة أو الناصر صلاح الدين مقارنة و مشاهدة

مشهد غايه في الضراوة للمخرج المبدع ريدلي سكوت في فيلم مملكة الجنة كيف قتل رينولد دوم
شوتيان رسول صلاح الدين و فصل رأسه ردا على طلب صلاح الدين جثمان أخته و رءووس من قتلوها و تسليم القدس بعد مهاجمة قافلة الحجاح و قتل أخت صلاح الدين ..

وهذا ما حدث بالفعل و الذي لم يتعرض له فيلم يوسف شاهين والذي أشار فقط لمهاجمة قافلة الحجاح ..كما انه حينما عرض المياه عليه بعد انتصار موقعة حطين الساحق و فصل رأس مساعده و أمر أخيه عادل بقطع رأسه فعلا لم يبارزه كما ادعى يوسف شاهين و لم تكن المبارزة مكتوبة في سيناريو السباعي و عبد الرحمن الشرقاوي و لكن يوسف شاهين أصر عليها في فانتازيا خاصة له ..نقل ريدلي سكوت وقائع تاريخية دقيقة ولكنه فبرك شخصية الفارس الحداد (اورلاندو بلووم) والذي ربما كان أمير الكرك قبل 200 سنة من صلاح الدين ولكن سكوت قال انا صانع أفلام و لست مؤرخ أدبي و العمل الدرامي يلزم معركة متكافئة تحبس الانفاس و تذبذب الموازين في النهاية و تخرج المشاهد حائرا من المنتصر و المهزوم و تاريخ صلاح الدين يوحى بانتصارات ساحقة حتى مشهد الأبراج فهي لم تكن مع صلاح الدين و لا مع ريتشارد كما ادعى يوسف شاهين و اول من وقف أمامها كان نجم الدين الأيوبي في معركة المنصورة و حملة لويس التاسع ..اختصر سكوت قرابة الاربعين دقيقة من مشاهد المعارك في الفيلم لأنه سيكون مبهرا لانتصارات عربية خصوصا ان عرض الفيلم كان بعد 11 سبتمبر أما عن شخصية عيسى العوام فقد كان مسلما ولم يكن نصرانيا و بالفعل تزوج من فارسة صليبية دخلت الاسلام لانها لم تكن تستطيع الحياة خارج القدس و تعرض الفيلم لانتقادات أكاديمية كثيرة و تفوقت ليلى فوزي في دور فيرجينيا و التي هي سيبيليا حقيقة ولكن اختاروا أسماء سهلة للمشاهد العربي ورأى البعض ان بلووم كان ضعيفا في دور الفارس الحداد برغم حصولة على جائزتين…
والاسلام انطلق من نقطة مكة و من حول المسجد الحرام و كعبة نبي الله ابراهيم و اسماعيل ومن أرض صحراء شاسعة قاحلة ووادي بغير ذي زرع فقط كعبة ابراهيم و بئر زمزم لا مدرسة و لا مصنع و لا علوم و لا فنون غير الشعراء و تجارة الشتاء و الصيف وديانة حرفت ملة ابراهيم لله حنيفا و اتخذت من تماثيل اللات و العزة و مناة آلهة تقربهم الى الله ..
ديانة في غاية السذاجة بلا فلسفة و لا منطق
في الوقت الذي كانت فيه أوروبا أومستبدين و محاربين الروم يستولون على كل شئ ويهتكون حرمات كل شئ باجرام و بطش بلا رحمة و لا هوادة و باسم الصليب والمسيح..وفي هذه الأجواء التي تعصف بالبشرية
و في هذه الأرض الصحراوية الفقيرة ولد محمد بن عبد الله نور الله في الأرض في الوقت الذي رسخ فيه هرقل عظيم الروم للعقيدة الايريسية والتثليث نسبة لايريوس
و في سنة الهجرة الى المدينة ومع شدة اضطهاد المسلمين .. غلبت الروم (حاليا أوروبا و أمريكا= الكاثوليكية البروتستانية العلمانية الملحدة) من الفرس (حاليا ايران وتابعتها روسيا الشيعية الارثودوكسية العلمانية الشيوعية الملحدة ) والتي كانت تحكم من قبل كسرى الثاني و تدين بديانة الزراداشية و التي تؤله كسرى ذاته – غلبت الروم في أدنى الأرض وبعد غلبهم غلبوا مرة أخرى
ومع صلح الحديبية يرسل رسول الله رسالة الى هرقل الفيلسوف الفارس و المحارب المنتصر ليدعوه للاسلام و الا فانه يحمل اثم و ذنب الايريسين
ثم لتفتح القدس موحدة باسم الله في زمن عمر بن الخطاب …
ثم يعود أهل الكتاب هودا و نصارى ليتجمعوا في النقطة ذاتها وقت هوان المسلمين و تفرقهم
ثم ليكون انتشار الاسلام القادم يقينا لأهل الكتاب خاصة من هذه الأرض المباركة و التي ستشهد حربا ضارية قادمة حتمية لتصحيح مفاهيم ضللت شعوب الأرض قرونا طويلة وأماتت الكثير منهم على باطل و عاشت شعوبا على باطل و لا تزال ترصد المليارات و تدشن الفضائيات لتبقي الناس في ضلال.. وتستمر عبوديتهم بلا هواده..و غدا لناظره قريب
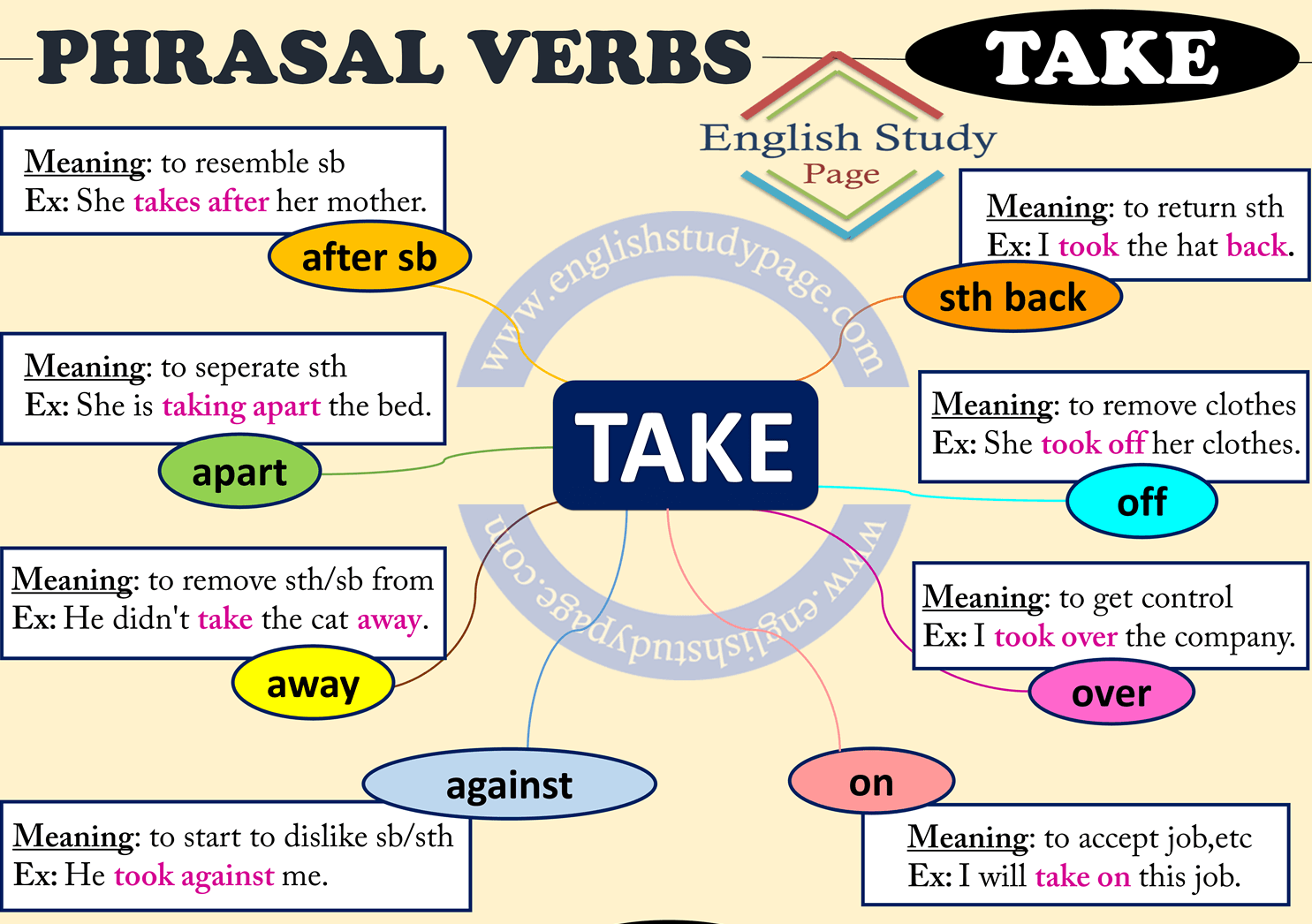
IMPROVE YOUR ENGLISH IN A MINUTE= TAKE
Energize yourself

Pace yourself.

Instead of burning through all your battery life in two hours, spread it out between morning tasks, afternoon tasks, and evening activities — with rest and meals in between. Consider these strategies to get the most mileage from your battery.
Take a walk or a nap.

A short power nap can restore energy, but if you struggle to get enough sleep at night, napping can make insomnia worse. Rather than take a siesta, get moving. Get up and walk around the block, or just move around. If you are not an insomniac, though, enjoy that 20- to 30-minute power nap.
Skip most supplements.

There is no evidence that energy-boosting or “anti-aging” supplements work. In particular:
DHEA. There is absolutely no evidence that that DHEA provides any benefit. And you especially shouldn’t be buying it from ads in the back of a magazine, because you don’t know what’s in it.
Iron.

Iron is only beneficial if you are clearly deficient, which a doctor can check with a blood test. Unless you are low in iron, you don’t need to take it, and getting too much iron can be harmful.
B vitamins.

It is true that B vitamins (B1, B2, B6, B12) help the body convert food into the form of energy that cells can burn, but it’s a myth that taking in more B vitamins supercharges your cells.
Eat long-lasting fuel.

Your body burns through sugars and highly processed carbohydrates, like white bread, white rice, or prepared bakery goods, more rapidly than protein and the carbohydrates in whole grains. Instead, try yogurt with a sprinkling of nuts, raisins, and honey. Your body will take in the carb-fiber-protein mix more gradually. To really sustain yourself over the course of the day, eat a breakfast and a lunch that include complex carbohydrates and protein.
Don’t skip meals.

It’s better to evenly space your meals out so your body gets the nourishment it needs all through the day.
من يدعي النبوة و المجنون ؟
الألفاظ الإهتزازية في القرآن الكريم

هل تعلم ما هي الألفاظ الإهتزازية في القرآن الكريم ؟
– عندما أخبرنا الله جلّ وعلا عن الأرض ؛
• { إذا زلزلت الأرض زلزالها }
تأمل لفظة ( زل زل ) فهي تكرار حرفين !
– وعندما يغضب الله تعالى على قوم صالح الذين عصوا أمر الله ورسوله وعقروا الناقة تأتي لفظة ؛
• { فدم دم عليهم ربهم }
فتأمل دم دم !
– وعندما تنكشف الحقيقة وبقوة عن ظلامة يوسف الصديق لعشر سنوات يقبع فيها في السجن ظلما من قبل زليخا تأتي لفظة ؛
• { الآن حص حص الحق }
فتأمل حص حص !
– وعندما يتحدث القرآن عن حدث مهم تقشعر له الأبدان يوم القيامة تأتي لفظة
• { إذا دكت الأرض دكا دكا * وجاء ربك والملك صفا صفا }
تأمل !
– وعندما يتحدث القرآن عما أعدّ ﻷهل الجنة من نعيم تأتي لفظة ؛
• { متكئين على رف رف خضر وعبقري حسان }
فتأمل !
– وعندما يتحدث عن شدة ظلمة الليل تأتي لفظة
• { والليل إذا عس عس }
كذلك تأمل !
فتتجلى الروعة القرآنية من هذه الكلمات المؤثرة …
وهذا يسمى في روائع بلاغة القرآن الكريم :-
( الألفاظ الاهتزازية )
وهي ألفاظ تشعرك بشدتها وقوتها واهتزازها من خلال تكرار حرفين متتاليين أو تكرار كلمة كاملة قوية اهتزازية لبيان أحداث في غاية الأهمية
فسبحانك ربنا ما قدرناك حق قدرك …
وهل تعلم ما هي الخماسيات …
من دقة القرآن الكريم تلك الخماسيات التي جعلها الله في كتابة في افتتاحيات السور لتسهيل معرفة بدايات السور في القرآن الكريم وتشمل الفئات السبع التالية :
الفئة الأولى :
خمس سور مفتتحة بالتحميد :
الفاتحة، الأنعام، الكهف، سبأ، فاطر
وكلها مكية …
الفئة الثانية :
خمس سور مفتتحة بالتسبيح :
الحديد، الحشر، الصف، الجمعة، التغابن
وكلها مدنية …
الفئة الثالثة
خمس سور مفتتحة بألف لام راء
يونس، هود، يوسف، إبراهيم، الحجر
وكلها مكية …
الفئة الرابعة
خمس سور مفتتحة بالنداء
النساء، المائدة، الحج، الحجرات، الممتحنة
وكلها مدنية
الفئة الخامسة
خمس سور مفتتحة بنداء الرسول ﷺ
الأحزاب، الطلاق، التحريم، المزمل، المدثر
وكلها مكية
الفئة السادسة :
خمس سور مفتتحة بالاستفهام :
الإنسان، الغاشية، الشرح، الفيل، الماعون
وكلها مكية
الفئة السابعة
خمس سور مفتتحة بالأمر
الجن، الكافرون، الإخلاص، الفلق، الناس
وكلها مكية
Steps to Overcome Social Anxiety

What is social anxiety?
Social anxiety is when you feel nervous, tense or uncomfortable in social situations because you’re worried other people are judging you. Almost everyone has experienced social anxiety at one point or another. Life is rife with moments of self-consciousness–from job interviews to first dates, we all occasionally feel nervous around other people. But social anxiety becomes a problem when it’s so frequent or intense that it gets in the way of important things in your life. You might not apply for a dream job because it requires an interview, or you might find it hard to be around even family and friends because you’re so worried about what they think of you.
If social anxiety has prevented you from doing the things you want, such as making new friends or going on dates, you’re not alone. Social anxiety is one of the most common mental health conditions in the United States, affecting 15 million adult Americans each year.
Recognizing if you have social anxiety
While social anxiety always involves a fear of being judged negatively, the actual situations that cause it can vary greatly from person to person. Many people with social anxiety feel nervous in most situations that involve interacting with or performing in front of other people. But some people only experience social anxiety in particular situations, such as speaking in front of others or hosting an event. For example, a person who is typically very outgoing and comfortable talking to strangers at parties might only have social anxiety when giving presentations. In fact, public speaking is one of the most common specific forms of social anxiety.
Common situations in which people experience social anxiety:
- Speaking in front of a group
- Talking to strangers
- Being the center of attention (such as when you are hosting a dinner)
- Speaking to authority figures (such as your boss)
- Answering the phone
- Eating or drinking in front of others
- Talking to someone you find attractive
Signs and Symptoms of Social Anxiety
People often think social anxiety is just a feeling, but it actually has four components: thoughts, feelings, physical sensations and behaviors. Most people might begin recognizing their social anxiety when they notice nervousness also is accompanied by physical symptoms such as trembling and crying. When you’re anxious, the four components interact with and build upon each other, causing a cycle of anxiety. For example, here’s how your anxiety might manifest itself if you’re nervous about giving a presentation at work:
Thoughts:

Often, your anxiety will begin with a negative thought, such as “I’m going to screw up” or “People will think I’m stupid.”
Feelings:

These thoughts cause you to feel negative emotions, such as stress or worry.
Physical Response:
 Your body reacts to your negative thoughts and feelings with a physical response, such as blushing, sweating or shaking.
Your body reacts to your negative thoughts and feelings with a physical response, such as blushing, sweating or shaking.
Behaviors: You try reducing your anxiety with conscious or unconscious actions, such as averting your gaze or hiding behind the podium (to prevent people from seeing you shake). Acting this way may make you think everyone else notices you look stiff (an anxious thought), which then can cause you to feel even more stressed (an anxious feeling).
People with social anxiety often don’t realize when their behavior is being driven by anxiety. People with social anxiety tend to exhibit three types of behaviors:
- Avoidance behaviors: When you stay away from situations that make you anxious. For example, you might turn down opportunities to give presentations at work.
- Escape behaviors: When you leave situations that make you anxious, such as leaving a concert or party after just a few minutes because of your anxiety.
- Safety behaviors: Actions you take to reduce your anxiety in social situations, such as drinking to feel more comfortable or playing a game on your phone at lunch. In the example above, averting your gaze or hiding behind the podium during the presentation are safety behaviors.
What to do if you have social anxiety
If you think you have social anxiety, the most important question to ask yourself is whether it prevents you from achieving your goals. For example, we mentioned earlier that a large majority of people report a fear of public speaking. You might be one of them. But if your job or goals don’t require public speaking, then being afraid of it might not be a big deal. On the other hand, if your fear is keeping you from getting the promotion you want, or getting in the way of an important personal goal, such as giving a speech at your sister’s wedding, then you might consider looking for help.
The cognitive part of CBT is based on the idea that it’s not a social situation that makes you anxious, but your interpretation of that situation. For example, if you’re having dinner with a friend and she leaves early, you can interpret these several ways. You might think she found dinner with you boring (leading you to feel anxious), or you might think she had a long day and was tired (and feel neutral). People with social anxiety tend to interpret situations in a disproportionately negative way. CBT teaches you to recognize and embrace the existence of alternative interpretations, allowing you to identify if other possible explanations are less likely to trigger your anxiety.
The behavioral part of CBT involves gradually facing the situations that make you anxious to overcome your fear of them. (This exercise is called an “exposure.”) You probably imagine the worst-case scenario will happen if you confront these situations, so you tend to avoid them. However, when you actually place yourself in the situations you fear, you have two critical realizations: First, the bad outcome you fear happens less often than you think. Second, even if it does happen, you can handle it. It’s key that exposures are gradual: You start small, with a situation that causes some anxiety but is doable. Then work your way up to situations that make you really anxious.
For example, if giving a presentation makes you extremely anxious, to the point where you might even call in sick to avoid it, your first exposure would be a similar but less anxiety-inducing situation, such as telling a story to a group of friends. Once you learn to get comfortable in these practice situations, you’ll be able to take your newfound confidence to more difficult situations you greatly fear or have been avoiding.
Tips for People with Social Anxiety
Here are some CBT-based tips for dealing with social anxiety at the moment:
- Remember everyone is self-conscious.
 Social anxiety is common, and many people experience it. If you’re at a party and feel really anxious about introducing yourself to new people, remember that other people might feel the same way.
Social anxiety is common, and many people experience it. If you’re at a party and feel really anxious about introducing yourself to new people, remember that other people might feel the same way.
- Pause to examine the evidence.
 When you’re feeling anxious, take a moment and try identifying the anxious thoughts running through your head. Challenge them by asking questions such as: “What evidence do I have this is true?” and “Is there another explanation for what happened?” If someone responds curtly to you, you may have the anxious thought that “They think I’m boring.” What if you challenged that thought and instead considered another explanation: Maybe they were in a hurry, or maybe they were already on their way to talk to someone else when you approached them.
When you’re feeling anxious, take a moment and try identifying the anxious thoughts running through your head. Challenge them by asking questions such as: “What evidence do I have this is true?” and “Is there another explanation for what happened?” If someone responds curtly to you, you may have the anxious thought that “They think I’m boring.” What if you challenged that thought and instead considered another explanation: Maybe they were in a hurry, or maybe they were already on their way to talk to someone else when you approached them.
- Imagine the worst-case scenario. Often, people with social anxiety think making a mistake will cause far worse consequences than it actually would. If you’re worried about something, such as stumbling over your words, ask what really would happen if you stumbled over your words. Would people really laugh at you? They’d probably barely notice it or quickly forget about it and continue the conversation.

- Remind yourself anticipation is worse than reality.
 Often, our worries about an upcoming situation are worse than the situation itself. If you’re worried about striking up a conversation because you think you’ll have nothing to say, remind yourself that you only have to start with “Hello.” Once you begin the conversation, it gets a lot easier.
Often, our worries about an upcoming situation are worse than the situation itself. If you’re worried about striking up a conversation because you think you’ll have nothing to say, remind yourself that you only have to start with “Hello.” Once you begin the conversation, it gets a lot easier.
- Bring a cheat sheet. Before going into an anxiety-inducing situation, anticipate what anxious thoughts you’ll have and challenge them on a piece of paper. Bring this piece of paper with you to the event (or save it on your phone). Then if you start feeling nervous, you can look at it to remind yourself of your thought challenges and calm yourself down.

- Consider getting help. If you find social anxiety really is impacting your life (For instance, getting in the way of your career or relationships, or making it hard to go to social events you want to attend.), consider seeking help through an evidence-based solution such as CBT.

We get lots of questions about social anxiety. People want to know if everyone feels the way they do or if their social habits are ‘normal.’ I also know that some forms of social anxiety are beyond the advice on this blog. Since I am not an expert in social anxiety, I found someone to tackle this topic for us. Joyable is an online service to help tackle social anxiety. I was unsure of what to expect at first, but after completing the entire program, I was blown away. After I finished the program, I reached out to them to do a guest post for our blog on social anxiety and how Joyable helps.
Just to be clear, they are not a sponsor, they are not paying for this coverage and I get no benefit if you use Joyable. I am posting this because I think their perspective is really interesting and I think it can help people—it helped me. They have been wonderful and put together this great post for us. I hope you enjoy it and please let me know if you end up using Joyable and what you think.
Don’t Diet and loose weight

If you’re struggling to lose weight, you probably feel like the odds are stacked against you. You’re not necessarily wrong.
“There is so much great-tasting food, and it’s abundant and in your face all the time. To me it’s kind of a miracle that people aren’t even heavier than they are. In addition to an abundance of food, most people today also have a far more sedentary lifestyle than past generations. “Even active people who exercise a lot aren’t expending the calories their ancestors did.
So, while losing weight is simple in theory — reduce your calorie intake — it’s not easy in practice.
If you put people into a locked metabolic ward and feed them only 60% of their usual caloric intake, they will lose weight. But for free-living people that’s really hard.
But as hard as it is to shed pounds, the bigger challenge may await if you are successful.
It is relatively more difficult to maintain the loss.
This is particularly true for women after menopause. “When people get older, it becomes difficult to dissipate the energy from foods. They need to modify their eating habits — to follow healthier patterns. It’s challenging to change any habits, including eating habits.
People today view food as far more than just sustenance.
Eating is a source of gratification; it’s a social activity; it’s a reward.
This is why many diets work in the short term but fail later on.
Many diets are a radical shift from what people normally eat, and this is not sustainable.
But don’t throw your hands up and resign yourself to keeping those extra pounds. There are strategies that can help you chip away at excess weight. Below are some simple tips that you can use to get the scale moving in the right direction — and keep it there.
Don’t diet; improve your diet.

Don’t focus your eating solely on weight loss; focus on overall health. Follow a diet that is rich in fruits, vegetables, and healthy fats. “Even today, after all the data that we have, people still think that eating fat makes them fat, and they try to find low-fat products,” says Dr. Stampfer. “That has been very well debunked. Eating fat doesn’t make you fat. There are good studies that show eating healthy fats helps people control their weight better than diets than exclude them.”
Overall, choosing a sustainable diet that is focused on health and not just weight can help you make lasting improvements. “Adopt a healthy diet, and eat just a little bit less,” says Dr. Stampfer.
Exercise regularly.

This has been said a million times, but it can’t be emphasized enough: boosting your activity level can help you lose weight and keep it off. “For most people, long-term weight control is hard without some physical activity,” says Dr. Stampfer.
Your metabolism slows with age, which means you burn fewer calories to keep basic body functions going. At the same time, bone and muscle mass decline and fat mass increases. This insidious pattern happens naturally as you get older unless you take steps to avoid it.
“I’m a strong advocate of not a just aerobic activity but also weight training and calisthenics,” says Dr. Stampfer. “Muscle building can not only bring up your body’s metabolic rate but also bring its own distinct health benefits that are often not as well appreciated as those associated with an aerobic activity.”
Try a variety of strategies.

Different diets work for different people. Sometimes finding the right strategy takes trial and error. One approach that holds promise for many is mindful eating — taking the time to stop and really focus on and enjoy your food. “The scientific evidence to my eye is meager, but I like the concept,” “We’ve all had that experience of eating a bowl of something and not even remembering having eaten it.”
Another simple trick is to put your fork down between bites instead of holding it in your hands. Pick it up when you are going to take the next bite.
Persevere.
Losing weight is really hard to do, and many people fail many times before they succeed. Don’t give up. Each day, commit to eating a little bit less.
If you go off track, recommit the following day and keep at it over time.
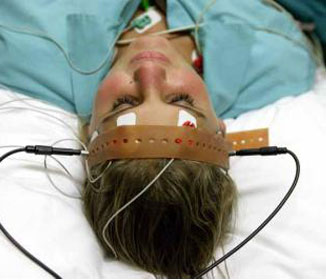
Electro-Convulsive therapy : Facts and Myths
As evidence supporting the use of
electroconvulsive therapy (ECT)
to treat patients with depression
and other psychiatric illnesses continues
to grow, myths about this treatment
persist. In light of these myths, patients
might be reluctant to receive ECT. As clinicians,
we need to educate patients about
the safety and effectiveness of this treatment.
Here are 10 of the most commonly
held myths about ECT, and why each is a
misconception.
1. It is a barbaric treatment. ECT is conducted
in a controlled medical environment,
either during a hospitalization or as
an outpatient procedure, by a team, consisting
of a psychiatrist, anesthesiologist,
and nurse. Patients receive a short-acting
intravenous anesthetic to ensure that they
are unaware of the procedure, and a muscle
relaxant to help prevent physical injury.
Vital signs and brain waves are monitored
throughout the procedure, which typically
lasts 15 to 20 minutes. Patients remain
relaxed, are unaware that they are having a
seizure, and experience no pain. Following
ECT, the patient is taken to a recovery area,
where he or she is closely monitored as the
medications wear off.
2. It causes brain damage. Studies using
MRI to look at the brain before and after
ECT have found no evidence that ECT
causes negative changes in the brain’s
structural anatomy.1
To the contrary, there
is evidence that there is neuroplasticity in
the brain in response to ECT, and the neurotrophin
brain-derived neurotrophic factor
also may be increased.2,3
3. It causes permanent memory loss.
ECT can result in both anterograde and
retrograde memory impairment; however,
anterograde amnesia typically lasts only
days to weeks. Retrograde amnesia is much
less common, but when it occurs, it tends
to be a loss of memory of events that took
place in the weeks leading up to and during
treatment. Using an ultra-brief (as opposed
to standard brief,) pulse, as well as right
unilateral (as opposed to bilateral) electrode
placement substantially reduces the risk of
cognitive and memory adverse effects.4
4. It is a treatment of last resort. Typically,
ECT is used for patients who have not
responded to other interventions. However,
ECT can be used as a first-line treatment
for patients if a rapid or higher likelihood
of response is necessary, such as when a
a patient is suicidal, catatonic, or malnourished
as a result of severe depression.5
5. It only works for depression. Evidence
shows ECT is efficacious for several psychiatric
conditions, not just unipolar depressive
disorder. It can effectively treat bipolar
depression, mania, catatonia, and acute
psychosis associated with schizophrenia
6. It is not safe. Death associated with
ECT is extremely rare. A recent analysis
estimated that the rate of ECT-related
mortality is 2.1 deaths per 100,000 treatments.
In comparison, the mortality rate
of general anesthesia used during surgery
has been reported as 3.4 deaths per
100,000 procedures.8
Evidence also suggests
ECT can be safely administered to
patients who are pregnant.9
7. It cannot be given to patients with epilepsy.
There are no absolute contraindications
to using ECT for these patients. Most
patients with epilepsy can be successfully
treated with ECT without requiring an
adjustment to the dose of their antiepileptic
medications.10
8. It will change one’s personality. ECT
has not been found to cause any alterations
in personality. Patients who are treated
with ECT may describe feeling more like
themselves once their chronic symptoms of
depression has improved. However, ECT
has not been shown to effectively treat the
symptoms or underlying illness of personality
disorders and it may not be an effective
treatment for depression associated with
borderline personality disorder.11
9. Its success rate is low. ECT has the highest
response and remission rates of any
a form of treatment used for depression.
An estimated 70% to 90% of patients with
depression who are treated with ECT show
improvement.12
10. It is a permanent cure. ECT is not likely
a permanent solution for severe depression.
The likelihood of relapse in patients with
severe depression who are helped by ECT
can be reduced by receiving ongoing antidepressant
treatment and some patients may
require continuation or maintenance ECT.13
References
1. Scott AI, Turnbull LW. Do repeated courses of ECT cause
brain damage detectable by MRI? Am J Psychiatry. 1990;
147(3):371-372.
2. Sartorius A, Demirakca T, Böhringer A, et al.
Electroconvulsive therapy increases temporal gray matter
volume and cortical thickness. Eur Neuropsychopharmacol.
2016;26(3)506-517.
3. Bocchio-Chiavetto L, Zanardini R, Bortolomasi M et al.
Electroconvulsive therapy (ECT) increases serum brain-derived
neurotrophic factor (BDNF) in drug resistant
depressed patients. Eur Neuropsychopharmacol. 2006;16(8):
620-624.
4. Sackeim HA, Prudic J, Nobler MS, et al. Effects of pulse
width and electrode placement on the efficacy and
cognitive effects of electroconvulsive therapy. Brain
Stimul. 2008;1(2):71-83.
5. American Psychiatric Association. The practice of
electroconvulsive therapy: recommendations for treatment,
training, and privileging: a task force report of the American
Psychiatric Association, 2nd edition. Washington, DC:
American Psychiatric Association; 2001.
6. Fontenelle LF, Coutinho ES, Lins-Martins NM, et al.
Electroconvulsive therapy for obsessive-compulsive
disorder: a systematic review. J Clin Psychiatry. 2015;76(7):
949-957.
7. Narang P, Glowacki A, Lippmann S. Electroconvulsive
therapy intervention for Parkinson’s disease. Innov Clin
Neurosci. 2015;12(9-10):25-28.
8. Tørring N, Sanghani SN, Petrides G, et al. The mortality
rate of electroconvulsive therapy: a systematic review and
pooled analysis. Acta Psychiatr Scand. 2017;135(5):388-397.
9. Sinha P, Goyal P, Andrade C. A meta-review of the safety
of electroconvulsive therapy in pregnancy. J ECT. 2017;33(2):
81-88.
10. Lunde ME, Lee EK, Rasmussen KG. Electroconvulsive
therapy in patients with epilepsy. Epilepsy Behav. 2006;
9(2):355-359.
11. Feske U, Mulsant BH, Pilkonis PA, et al. Clinical outcome
of ECT in patients with major depression and comorbid
borderline personality disorder. Am J Psychiatry. 2004;
161(11):2073-2080.
12. Kellner CH, McClintock SM, McCall WV, et al; CORE/
PRIDE Group. Brief pulse and ultrabrief pulse right
unilateral electroconvulsive therapy (ECT) for major
depression: efficacy, effectiveness, and cognitive effects. J
Clin Psychiatry. 2014;75(7):777.
13. Jelovac A, Kolshus E, McLoughlin DM. Relapse following
successful electroconvulsive therapy for major depression:
a meta-analysis. Neuropsychopharmacology. 2013;38(12):
2467-2474.
An estimated
70% to 90% of
patients with
depression who
are treated
with ECT show
improvement
Discuss this article at
www.facebook.com/
MDedgePsychiatry
continued from page 9
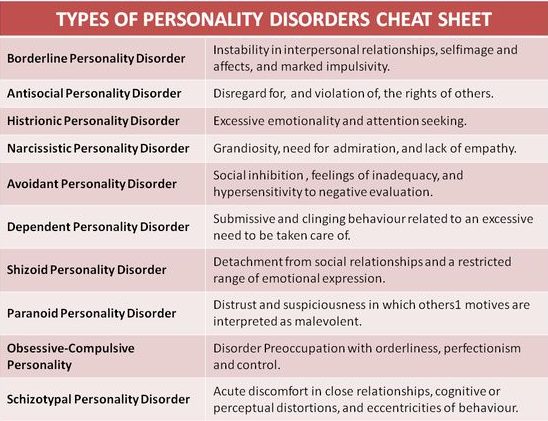
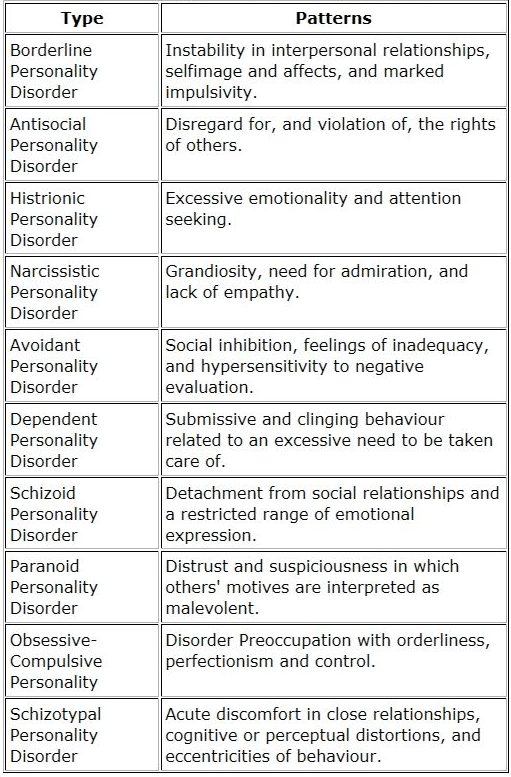
Personality disorders one sheet

If personality is the cluster of traits which form the uniform of the one either he or She. Magnified certain traits in one person can be disturbing others but the person himself/herself might not feel disturbed. Here is the sum of personality disorders cluster traits.
The same texts in different forms
ألعاب التوازن لطفلك
يمكنك ان تساعد طفلك لاكتساب الثقة بالسيطرة على توازنه و الثبات الحركي و الانفعالي مما يؤهله للمناخ المدرسي و التعلم الناجح .
ألعاب التوازن تساعدك لتنمية مهاراته كن مبتكرا و مساعدا له لاكتساب المزيد من قدرات التوازن و الثبات
و يمكنك ان تتناقش معه في قصة صغيرة و لا تمل من مشاهدتها عشرات المرات

ويمكنك ان تغني و ترقص معه و تعلمه العد و الاعداد
The ants go marching learn counting
Inflammation meaning and control
Heart disease. Rheumatoid arthritis. Diabetes. Alzheimer’s. These and other chronic diseases, affecting the lives of millions of Americans, have something in common — do you know what it is?
The answer is inflammation. What’s MEANT, and how can you deal with inflammation.
How inflammation attacks your health? To explain and simplify, there are two kinds of inflammation — acute (short-term) and chronic (long-term). While acute inflammation is a beneficial part of the healing process, chronic inflammation is linked to many serious health conditions. In the guide you’ll learn all about the dangers of chronic inflammation — for example:
The key role inflammation plays in cardiovascular disease, obesity, diabetes, metabolic syndrome, inflammatory bowel disease, and other chronic illnesses.
Inflammation and allergies. Sometimes the immune system becomes hypersensitive to allergens like pollen, dust, and animal dander, resulting in inflammation. The guide looks at the connection between inflammation and two common allergic conditions in particular — asthma and eczema.
There is a connection between diseases of the joints and inflammation, as well as the prominent role that inflammation plays in rheumatoid arthritis.
Inflammation and your brain. Inflammation also affects cognitive health, as it leads to the creation of damaging proteins associated with Alzheimer’s. The guide helps you understand the latest findings
How you can prevent and reduce inflammation
You can take control of chronic inflammation. One option is medication. Nonsteroidal anti-inflammatory drugs (such as aspirin and ibuprofen), known as NSAIDs, can help relieve inflammation. The report goes over these and other medicines, along with their benefits and risks.
You should learn about foods with powerful anti-inflammatory properties, such as fruits, vegetables, nuts, and fish. In addition, the report suggests lifestyle choices, like exercising, quitting smoking, and getting more sleep, which can help keep inflammation at bay.
Inflammation is the most dangerous condition your body has to handle to make you well and keep you that way. It diminishes your immune system. It can trigger a wide variety of serious degenerative illnesses, from early aging and heart disease to diabetes, arthritis, food intolerance and mental disorders. Inflammation is your body’s natural response to infection, injury and tissue damage. It comes in two forms: Acute and chronic inflammation—systemic inflammation, which spreads throughout your body. Acute inflammation is temporary, the purpose of which is to restore good tissue function as soon as possible. Your body creates inflammation as its defense against disturbing homeostasis in an attempt to prevent harm to surrounding tissues. Chronic inflammation is different. It turns into a festering fire causing pain, illness, and disability all round. The reactions it brings about in the body are highly complex, involving many cellular and molecular distortions. It acts upon pro-inflammatory immune cells that circulate throughout your body, damaging healthy areas like the linings of your blood vessels in arteriosclerosis, joint tissue in arthritis, gut mucosa in lactose and gluten intolerance, and pancreatic tissue in diabetes. It can even act as a precursor to cancer.
SURPRISING DISCOVERY
 Recently, highly respected cardiologists have pointed out that when it comes to the treatment of many conditions—such as heart disease—the medical profession has been doing it all wrong. Prescribing drugs to lower cholesterol, and telling people to restrict quality fats, do not protect from heart disease as we have been taught. The statins which cardiologists continue to prescribe are not only useless, they say, these pharmaceuticals can be seriously detrimental to your health. It is, they have discovered, inflammation in the arteries that is the real cause of arteriosclerosis and heart problems. Cholesterol can never line artery walls causing heart attacks and strokes unless systemic inflammation is widespread in your body.
Recently, highly respected cardiologists have pointed out that when it comes to the treatment of many conditions—such as heart disease—the medical profession has been doing it all wrong. Prescribing drugs to lower cholesterol, and telling people to restrict quality fats, do not protect from heart disease as we have been taught. The statins which cardiologists continue to prescribe are not only useless, they say, these pharmaceuticals can be seriously detrimental to your health. It is, they have discovered, inflammation in the arteries that is the real cause of arteriosclerosis and heart problems. Cholesterol can never line artery walls causing heart attacks and strokes unless systemic inflammation is widespread in your body.
Dwight Lundell, former Chief of Staff and Surgery at Banner Heart Hospital in Arizona, is one of many outspoken physicians in regard to this mistake. “We physicians with all our training, knowledge and authority often acquire a rather large ego that tends to make it difficult to admit we are wrong,” he says. “I freely admit to being wrong. As a heart surgeon with 25 years’ experience, having performed over 5,000 open-heart surgeries, today is my day to right the wrong with medical and scientific fact.”
THE TRIGGERS
 What causes inflammation in the body? Many things, from genetic inheritance to environmental influences—especially the wrong diet; being exposed to bacteria, inhalants, pollutants; even electromagnetic influences from cell phones, smart meters and towers; not to mention taking long-term courses of powerful drugs—from antibiotics to hormones, anti-depressants, analgesics and sedatives, to drugs like statins, commonly used to treat heart conditions; and other prescriptive drugs, the remains of which literally poison the body, badly polluting its terrain. If you wish to protect yourself from inflammation, you need to become aware of where it’s likely to be coming from. This means examining how you live your life, and making changes to protect yourself from possible causes. The second step is to learn about which foods cause inflammation and which foods can help protect you from it. Then it’s time to throw out every one of the inflammatory foods that line your cupboard and your refrigerator, and forever change how you may have been eating.
What causes inflammation in the body? Many things, from genetic inheritance to environmental influences—especially the wrong diet; being exposed to bacteria, inhalants, pollutants; even electromagnetic influences from cell phones, smart meters and towers; not to mention taking long-term courses of powerful drugs—from antibiotics to hormones, anti-depressants, analgesics and sedatives, to drugs like statins, commonly used to treat heart conditions; and other prescriptive drugs, the remains of which literally poison the body, badly polluting its terrain. If you wish to protect yourself from inflammation, you need to become aware of where it’s likely to be coming from. This means examining how you live your life, and making changes to protect yourself from possible causes. The second step is to learn about which foods cause inflammation and which foods can help protect you from it. Then it’s time to throw out every one of the inflammatory foods that line your cupboard and your refrigerator, and forever change how you may have been eating.
ANTI-INFLAMMATORY EATING
 Certain foods, herbs, spices, and supplements help reduce inflammation and protect your body from it in the future. Organic dark green vegetables are high on the list: Spinach, kale, dandelion greens, collard greens, broccoli, bok choy, beet greens, and asparagus are high on the list of protective vegetables. So are organic berries of all kinds, organic chicken, grass-fed lamb, beef, venison, wild salmon, and green-lipped muscles from New Zealand.
Certain foods, herbs, spices, and supplements help reduce inflammation and protect your body from it in the future. Organic dark green vegetables are high on the list: Spinach, kale, dandelion greens, collard greens, broccoli, bok choy, beet greens, and asparagus are high on the list of protective vegetables. So are organic berries of all kinds, organic chicken, grass-fed lamb, beef, venison, wild salmon, and green-lipped muscles from New Zealand.
Foods that cause inflammation which you want to avoid at any cost are all kinds of sugars, regardless of how much they may be promoted as “good for you”; all artificial sweeteners, which are chemically dangerous to your body; and all GMO foods, which can literally be deadly. A large percentage of the population also reacts badly to cow’s milk products—from the milk itself to cow’s yogurt and cheese. Another category of foods that can be highly inflammatory to the body are high-carbohydrate foods, from the common grains and cereals to packaged convenience foods which line your supermarket shelves. They are chock-full of colorants, flavor enhancers and other chemicals which poison your body. It goes without saying that you want to avoid all junk foods, from sugared drinks to pastries, completely. Explore instead using the faux grains, which do not pollute your body and are great for meals and baking.
SPICE IT UP
 Certain spices are wonderful for helping to quell inflammatory issues. Always buy organic. Most herbs in supermarkets have been irradiated—sprayed with herbicides and pesticides, which you do not want to allow into your body.
Certain spices are wonderful for helping to quell inflammatory issues. Always buy organic. Most herbs in supermarkets have been irradiated—sprayed with herbicides and pesticides, which you do not want to allow into your body.
- Turmeric has been used for centuries as a medicine for treating colds, flu, and liver disease. It contains curcumin which has been used for centuries to reduce inflammation.
- Cinnamon, in addition to its beautiful smell and flavor, has been shown in many studies to exert anti-inflammatory properties and to ease swelling.
- Garlic in fresh form eases the inflammation of arthritis, as well as helping to protect you from colds, flu, and other ailments.
- Ginger, in the form of a fresh root which you can grate into your foods and drinks, is fabulous for calming inflammation of upset stomachs, getting rid of headaches and infections.
- Cayenne, like other chili peppers, contains capsaicinoids which gives it its anti-inflammatory properties and can ease the pain of arthritis and headaches.
MAGNESIUM THE ULTIMATE
 For those in the know, it is magnesium that forms the foundation of both treatment and prevention of heart disease, arteriosclerosis and diabetes by calming the fires of chronic inflammation. Virtually everybody in the western world is seriously deficient in this wonderful mineral. All packaged convenience foods are very low in it. Magnesium deficiency is common in obesity, type 2 diabetes, and the insulin resistance that can trigger cardiac issues as well as the widespread incidence of cancer. Magnesium reduces hypertension, reduces your rate of aging, helps protect from bone fractures, and calms troubled minds. It is as basic as clean air and water for becoming healthy and staying healthy. There are many ways you can take magnesium, from swallowing supplements (not the best way) to bathing in magnesium chloride baths. One of the most effective ways to get more magnesium into your body—something all of us need to help clear inflammation and treat pain—is transdermal magnesium therapy.
For those in the know, it is magnesium that forms the foundation of both treatment and prevention of heart disease, arteriosclerosis and diabetes by calming the fires of chronic inflammation. Virtually everybody in the western world is seriously deficient in this wonderful mineral. All packaged convenience foods are very low in it. Magnesium deficiency is common in obesity, type 2 diabetes, and the insulin resistance that can trigger cardiac issues as well as the widespread incidence of cancer. Magnesium reduces hypertension, reduces your rate of aging, helps protect from bone fractures, and calms troubled minds. It is as basic as clean air and water for becoming healthy and staying healthy. There are many ways you can take magnesium, from swallowing supplements (not the best way) to bathing in magnesium chloride baths. One of the most effective ways to get more magnesium into your body—something all of us need to help clear inflammation and treat pain—is transdermal magnesium therapy.
Get yourself a spray bottle of high-quality magnesium chloride and spray it on your body, massaging it in all over. Magnesium chloride is taken right through your skin into the cells. Slowly but surely, doing this three times a day counters inflammation and pain superbly well. Spray it on or have a friend massage it into your body. When it dries, it may leave traces of white powder on the skin surface. This is nothing to worry about. It is some of the magnesium itself, that’s all; you can brush it off. Life Flo Health makes a pure Magnesium Chloride Oil, which is inexpensive. It provides 66mg of magnesium chloride for every 4 sprays or 560mg per teaspoon. It is taken from the Ancient Zechstein Seabed, which lies 1600 to 2000 meters beneath the surface of the earth in the Netherlands, and is 100% pure.
Magnesium chloride has no equal when it comes to the effectiveness of using magnesium to counter inflammation and athletic pain. It must be 100% pure magnesium chloride, not any other form of the mineral. I use it every day. Clearing inflammation from your body in whatever form it occurs may well be the very best action you can take to help you live a long and healthy life, during which you look and feel your very best at every age.
TOPIRAMATE
Topiramate
What’s of Interest:
- In 2014, Topamax (topiramate) became the first medication approved to prevent migraine headaches in adolescents (ages 12 to 17)
Brands
- Topamax, others
Class
- Anticonvulsant, voltage-sensitive sodium channel modulator
Approved For:
- Migraine prophylaxis (ages 12 and older)
- Other indications include partial onset seizures, primary generalized tonic-clonic seizures, seizures associated with Lennox-Gastaut Syndrome, and chronic weight management in obese or overweight adults (in combination with phentermine)
Dosing
Formulation:
- Tablet 25 mg, 50 mg, 100 mg, 200 mg
- Sprinkle capsule 15 mg, 25 mg
- An extended release capsule (25 mg, 50 mg, 100 mg, 200 mg) is also available; this formulation is not approved for migraine prophylaxis
Dosing Tips:
- Migraine: initial 25 mg/night for the first week; increase weekly in 25-mg increments; approved dose 100 mg/day in two divided doses
- For migraine, the individual dose may vary widely. Some patients benefit from doses as low as 25 mg/day but others may require much higher doses than the 100 mg/day approved for migraine prophylaxis
- Adverse effects may increase as dose increases
- Weight loss is often dose-related, but patients on lower doses (50 mg) still lose weight
- Slow titration minimizes sedation and other adverse effects
- Can be taken with or without food
- Sprinkle capsule formulation can be swallowed whole or sprinkled over approximately a teaspoon of soft food (e.g., applesauce); the mixture should be consumed immediately
- Headaches may return within days to months of stopping, but patients often continue to do well for 6 or more months after stopping
- Baseline and periodic serum bicarbonate levels to monitor for hyperchloremic, non-anion gap metabolic acidosis (i.e., decreased serum bicarbonate below the normal reference range in the absence of chronic respiratory alkalosis)
Pearls:
- Migraines may decrease in as little as 2 weeks but can take up to 3 months on a stable dose to see the full effect
- The goal when using topiramate for migraine prophylaxis is a 50% or greater reduction in migraine frequency or severity; consider tapering or stopping if headaches remit for more than 6 months or if considering pregnancy
- Augmenting options for a migraine include beta blockers, antidepressants, natural products, other anticonvulsants, and nonmedication treatments such as biofeedback to improve headache control
Children and Adolescents:
- Approved for use in adolescents ages 12 and older for migraine prophylaxis
- Approved for use in children age 2 and older for treatment of partial-onset seizures (adjunct and monotherapy), primary generalized tonic-clonic seizures (adjunct and monotherapy), and seizures associated with Lennox-Gastaut syndrome (adjunct only)
- Clearance is increased in pediatric patients
Pregnancy:
- Effective June 30, 2015, the US FDA requires changes to the content and format of pregnancy and lactation information in prescription drug labels, including the elimination of the pregnancy letter categories; the Pregnancy and Lactation Labeling Rule (PLLR or final rule) applies only to prescription drugs and will be phased in gradually for drugs approved on or after June 30, 2001
- Controlled studies have not been conducted in pregnant women
- Increased risk of cleft lip/palate
- Hypospadia has occurred in some male infants whose mothers took topiramate during pregnancy
- Patients with migraine should generally stop topiramate before considering pregnancy
- Migraine usually improves in the last 2 trimesters
- Antiepileptic Drug Pregnancy Registry: (888) 233–2334
Side Effects
Weight Gain:
Sedation:
Notable or Dangerous Side Effects:
- Sedation; cognitive problems, especially word-finding difficulties; mood problems
- Nausea, appetite loss, weight loss
- Taste perversion, pallinopsia (a rare visual disturbance that causes persistence of images; benign but frightening for the patient)
- Carbonic anhydrase inhibition can cause paresthesias and metabolic acidosis and may lead to kidney stones
- Secondary angle-closure glaucoma
- Oligohidrosis and hyperthermia (more common in children)
- Sudden unexplained deaths have occurred in epilepsy (unknown if related to topiramate use)
Drug Interactions:
- Carbamazepine, phenytoin, and valproate may increase the clearance of topiramate, and thus decrease topiramate levels, possibly requiring a higher dose of topiramate
- Lamotrigine, hydrochlorothiazide, and metformin may increase topiramate levels
- Topiramate can decrease levels of lithium, digoxin, valproic acid, and phenytoin
- Topiramate may increase levels of amitriptyline and metformin
- Topiramate may interact with carbonic anhydrase inhibitors to increase the risk of kidney stones
- Higher-dose topiramate (>200 mg) can decrease plasma concentrations of estrogens and progestins in patients taking oral contraceptives; a higher dose of estrogen or alternative methods of contraception should be considered
- Topiramate can interact with CNS depressants and alcohol with neuropsychiatric and cognitive consequences
Cardiac Impairment:
- No known effects
Renal Impairment:
- Topiramate is renally excreted, so the dose should be lowered by half
- Can be removed by hemodialysis; patients receiving hemodialysis may require supplemental doses of topiramate
Hepatic Impairment:
- Use with caution
OLANZAPINE

Olanzapine
What’s of Interest:
- US FDA warned that olanzapine is associated with a rare but serious skin condition known as Drug Reaction with Eosinophilia (DRESS). DRESS may begin as a rash but can progress to others parts of the body and can include symptoms such as fever, swollen lymph nodes, swollen face, inflammation of organs, and an increase in white blood cells known as eosinophilia. In some cases, DRESS can lead to death. Clinicians prescribing olanzapine should inform patients about the risk of DRESS; patients who develop a fever with rash and swollen lymph nodes or swollen face should seek medical care. Patients are not advised to stop their medication without consulting their prescribing clinician.
Brands
- Zyprexa, Zyprexa Relprevv, Olasek, other
Class
- Atypical antipsychotic (serotonin-dopamine antagonist; second-generation antipsychotic; also a mood stabilizer)
Approved For:
- Schizophrenia (ages 13 and older)
- Maintaining response in schizophrenia
- Acute agitation associated with schizophrenia (intramuscular)
- Acute mania/mixed mania (monotherapy and adjunct to lithium or valproate) (ages 13 and older)
- Bipolar maintenance
- Acute agitation associated with bipolar I mania (intramuscular)
- Bipolar depression [in combination with fluoxetine (Symbyax)]
- Treatment-resistant depression [in combination with fluoxetine (Symbyax)]
Dosing
Formulation:
- Tablets 2.5 mg, 5 mg, 7.5mg, 10 mg, 15 mg, 20 mg
- Orally disintegrating tablets 5 mg, 10 mg, 15 mg, 20 mg
- Intramuscular formulation 5 mg/mL, each vial contains 10 mg (available in some countries)
- Depot 210 mg, 300 mg, 405 mg
- Olanzapine-fluoxetine combination capsule (mg equivalent olanzapine/mg equivalent fluoxetine) 6 mg/25 mg, 6 mg/50 mg, 12mg/25 mg, 12 mg/50 mg
Dosage range:
- 10–20 mg/day (oral or intramuscular)
- 6–12 mg olanzapine /25–50 mg fluoxetine (olanzapine-fluoxetine combination)
- 210–300 mg/2 weeks (depot)
Dosing Tips–Oral:
- Initial 5–10 mg once daily orally; increase by 5 mg/day once a week until desired efficacy is reached; maximum approved dose is 20 mg/day
- More may be more: raising usual dose above 15 mg/day can be useful for acutely ill and agitated patients and some treatment-resistant patients, gaining efficacy without many more side effects
- Some heroic uses for patients who do not respond to other antipsychotics can occasionally justify dosing over 30 mg/day and short-term up to 90 mg/day
- For high doses in treatment-resistant or violent patients, monitor therapeutic drug levels and target generally higher than the usual range of 5–75 mg/mL (i.e., greater than 125 mg/mL), but keep below the toxic range associated with QTc prolongation (700–800 mg/mL)
- Rather than raise the dose above these levels in acutely agitated patients requiring acute antipsychotic actions, consider augmentation with a benzodiazepine or conventional antipsychotic, either orally or intramuscularly
- Rather than raise the dose above these levels in partial responders, consider augmentation with a mood-stabilizing anticonvulsant, such as valproate or lamotrigine
- Clearance of olanzapine is slightly reduced in women compared to men, so women may need lower doses than men
- Children and elderly should generally be dosed at the lower end of the dosage spectrum
- Treatment should be suspended if absolute neutrophil count falls below 1,000/mm3
Dosage Tips–Depot:
- Initial dose: 210–300 mg/2 weeks (depends on stabilizing oral dose)
- Maintenance dose: 210–300 mg/2 weeks (depends on stabilizing oral dose)
- Maximum recommended dose 300 mg every 2 weeks or 405 mg every 4 weeks
- Conversion from oral dose: if stable on 10 mg/day, then 210 mg LAI every 2 weeks or 405 mg LAI every 4 weeks for the first 8 weeks, then 150 mg LAI every 2 weeks or 300 mg LAI every 4 weeks
- If stable on oral 15 mg/day, then 300 mg LAI every 2 weeks for the first 8 weeks, then 210 mg LAI every 2 weeks or 405 mg LAI every 4 weeks
- If stable on oral 20 mg/day, then 300 mg LAI every 2 weeks
- Injection site: intramuscular gluteal
- Needle gauge: 19
- Injection volume: 150 mg/mL; range 1.0–2.7 mL
- Dosing schedule: 2 weeks, 4 weeks
- No oral supplementation required
- No leading required
- 3-hour post-injection monitoring required due to risk (0.2%) of post-injection delirium from vascular breach
Pearls
- Recent landmark head to head study in schizophrenia suggests greater effectiveness (i.e., lower dropouts of all causes) at moderately high doses compared to some other atypical and conventional antipsychotics at moderate doses
- Same recent head to head study in schizophrenia suggests greater efficacy but greater metabolic side effects compared to some other atypical and conventional antipsychotics
- Well accepted for use in schizophrenia and bipolar disorder, including difficult cases
- Documented utility in treatment-refractory cases, especially at higher doses
- Documented efficacy as augmenting agent to SSRIs (fluoxetine) in nonpsychotic treatment-resistant major depressive disorder
- Documented efficacy in bipolar depression, especially in combination with fluoxetine
- More weight gain than many other antipsychotics—does not mean every patient gains weight
- Motor side effects unusual at low-to-mid doses
- Less sedation than for some other antipsychotics, more than for others
- Controversial as to whether olanzapine has more risk of diabetes and dyslipidemia than other antipsychotics
- Cigarette smoke can decrease olanzapine levels and patients may require a dose increase if they begin or increase smoking
- A short-acting intramuscular dosage formulation is available
- A long-acting intramuscular dosage formulation is also approved
- Patients with inadequate responses to atypical antipsychotics may benefit from determination of plasma drug levels and, if low, a dosage increase even beyond the usual prescribing limits
- For treatment-resistant patients, especially those with impulsivity, aggression, violence, and self-harm, long-term polypharmacy with 2 atypical antipsychotics or with 1 atypical antipsychotic and 1 conventional antipsychotic may be useful or even necessary while closely monitoring
- In such cases, it may be beneficial to combine 1 depot antipsychotic with 1 oral antipsychotic
- Patients with inadequate responses to atypical antipsychotics may also benefit from a trial of augmentation with a conventional antipsychotic or switching to a conventional antipsychotic
- However, long-term polypharmacy with a combination of a conventional antipsychotic with an atypical antipsychotic may combine their side effects without clearly augmenting the efficacy of either
- Although a frequent practice by some prescribers, adding 2 conventional antipsychotics together has little rationale and may reduce tolerability without clearly enhancing efficacy
Children and adolescents:
- Approved for use in schizophrenia and manic/mixed episodes (ages 13 and older for both)
- Clinical experience and early data suggest olanzapine is probably safe and effective for behavioral disturbances in children and adolescents
- Children and adolescents using olanzapine may need to be monitored more often than adults
- Intramuscular formulation has not been studied in patients under 18 and is not recommended for use in this population
Pregnancy:
- Controlled studies have not been conducted in pregnant women
- There is a risk of abnormal muscle movements and withdrawal symptoms in newborns whose mothers took an antipsychotic during the third trimester; symptoms may include agitation, abnormally increased or decreased muscle tone, tremor, sleepiness, severe difficulty breathing, and difficulty feeding
- Psychotic symptoms may worsen during pregnancy, and some form of treatment may be necessary
- Early findings of infants exposed to olanzapine in utero currently do not show adverse consequences
- Olanzapine may be preferable to anticonvulsant mood stabilizers if treatment is required during pregnancy
- National Pregnancy Registry for Atypical Antipsychotics: 1-866-961-2388 or http://womensmentalhealth.org/clinical-and-research-programs/pregnancyregistry/
Side Effects
Weight gain:
Sedation:
Notable or dangerous side effects:
- Probably increases risk for diabetes mellitus and dyslipidemia
- Dizziness, sedation, weakness
- Dry mouth, constipation, dyspepsia, weight gain
- Peripheral edema
- Joint pain, back pain, chest pain, extremity pain, abnormal gait, ecchymosis
- Tachycardia
- Orthostatic hypotension, usually during initial dose titration
- Rare tardive dyskinesia (much reduced risk compared to conventional antipsychotics)
- Rare rash on exposure to sunlight
- Hyperglycemia, in some cases extreme and associated with ketoacidosis or hyperosmolar coma or death, has been reported in patients taking atypical antipsychotics
- Rare but serious skin condition known as Drug Reaction with Eosinophilia (DRESS)
- Rare neuroleptic malignant syndrome (much reduced risk compared to conventional antipsychotics)
- Rare seizures
- Increased risk of death and cerebrovascular events in elderly patients with dementia-related psychosis
Drug interactions:
- May increase effect of antihypertensive agents
- May antagonize levodopa, dopamine agonists
- Dose may need to be lowered if given with CYP450 1A2 inhibitors (e.g., fluvoxamine); raised if given in conjunction with CYP450 1A2 inducers (e.g., cigarette smoke, carbamazepine)
Cardiac impairment:
- Should be used with caution because of risk of orthostatic hypotension
Renal impairment:
- No dose adjustment required for oral formulation
- Not removed by hemodialysis
- For intramuscular formulation, consider lower starting dose (5 mg)
Hepatic impairment:
- May need to lower dose
- Patients with liver disease should have liver function tests a few times a year
- For moderate to severe hepatic impairment, starting oral dose 5 mg; increase with caution
- For intramuscuar formulation, consider lower starting dose (5 mg)
CLOZAPINE
Clozapine
What’s of Interest:
- Clozapine REMS and ANC monitoring update
Brands
- Clozaril, Leponex, Versacloz (oral suspension), Fazaclo ODT (oral disintegrating tablet)
Class
- Atypical antipsychotic (serotonin-dopamine antagonist; second-generation antipsychotic; also a mood stabilizer)
Approved For:
- Treatment-resistant schizophrenia
- Reduction in risk of recurrent suicidal behavior in patients with schizophrenia or schizoaffective disorder
Formulation:
- Tablet 12.5 mg, 25 mg scored, 50 mg, 100 mg scored
- Orally disintegrating tablet 12.5 mg, 25 mg, 50 mg, 100 mg, 150 mg, 200 mg
- Oral suspension 50 mg/mL
Dosing Tips:
- Initial 25 mg at night; increase by 25–50 mg/day every 48–72 hours as tolerated; obtain trough plasma level on 200 mg at bedtime
- The threshold for response is 350 ng/mL
- Median time to response after achieving therapeutic plasma levels of (350 ng/mL) is approximately 3 weeks; if there is no response after 3 weeks of therapeutic plasma levels, recheck plasma levels and continue titration
- Levels greater than 700 ng/mL are often not well tolerated
- No evidence to support dosing that results in plasma levels greater than 1,000 ng/mL
- Plasma half-life suggests twice daily administration, but in practice, it may be given once a day at night
- Doses greater than 500 mg per day may require a split dose
- Because of the monitoring schedule, prescriptions are generally given 1 week at a time for the first 6 months, then every 2 weeks for months 6–12, and then monthly after 12 months
- Lower ANC threshold for starting clozapine:
- General population: ≥1,500/µL
- Benign ethnic neutropenia (BEN): ≥1,000/µL
- If treatment is discontinued for more than 2 days, reinitiate with 12.5 mg once or twice daily; if that dose is tolerated, the dose may be increased to the previously therapeutic dose more quickly than recommended for initial treatment
- If abrupt discontinuation of clozapine is necessary, the patient must be covered for cholinergic rebound; those with higher clozapine plasma levels may need extremely high doses of anticholinergic medications to prevent delirium and other rebound symptoms
- Slow off-titration is preferred if possible to avoid cholinergic rebound and rebound psychosis
Contraindications:
- In patients with a myeloproliferative disorder
- In patients with uncontrolled epilepsy
- In patients with paralytic ileus
- In patients with CNS depression
- If there is a proven allergy to clozapine
NOTE THAT
• Clozapine is the gold standard treatment for refractory schizophrenia
• Clozapine is not used the first line due to side effects and monitoring burden
• In strictly-defined refractory schizophrenia, 50-60% of patients will respond to clozapine
• The response rate to another atypical antipsychotic in the refractory patient population ranges from 0–9%
• May reduce violence and aggression in difficult cases, including forensic cases
• Reduces suicide in schizophrenia
• May reduce substance abuse
• Little or no prolactin elevation, motor side effects, or tardive dyskinesia
• Cigarette smoke can decrease clozapine levels and patients may be at risk for relapse if they begin or increase smoking
• The US FDA has changed the requirements for monitoring, prescribing, dispensing, and receiving clozapine in order to address concerns related to neutropenia; in addition to updating the prescribing information for clozapine, the FDA has approved a new, shared risk evaluation and mitigation strategy (REMS)
• The Clozapine REMS program replaces the six existing clozapine registries, which are maintained by individual clozapine manufacturers. Prescribers, pharmacies, and patients will now be required to enroll in a single centralized program; patients already treated with clozapine will be automatically transferred. In order to prescribe and dispense clozapine, prescribers and pharmacies will be required to be certified in the Clozapine REMS Program.
Side Effects
Weight Gain:

Sedation:
Other Notable or Dangerous Side Effects:
- Orthostasis
- Slow titration
- Minimize use of other alpha 1 antagonists
- If orthostasis remains a problem, Florines 0.1–0.3 mg qd for volume expansion (contraindicated in congestive heart failure)
- Sialorrhea
- Atropine 1% drops, 1–3 drops sublingually at bedtime; can use up to 3 times per day if needed
- Ipratropium bromide 0.06% spray, 1–3 sprays intra-orally at bedtime; can use up to 3 times per day if needed
- Avoid use of systemic anticholinergic agents, which increase risk of ileus (benztropine, glycopyrrolate, etc.)
- Constipation, paralytic ileus
- Avoid psyllium as it may worsen symptoms
- All patients should receive docusate 250 mg when starting clozapine
- If needed, add Miralax 17 g
- If docusate + Miralax are ineffective, add either bisacodyl or sennosides
- If constipation still remains a problem, prescribe lubiprostone 8–24 mcg twice per day
- Sedation
- Slow titration
- Take at bedtime
- Tachycardia
- Atenolol 12.5 mg QD, increase to keep resting HR<100 bpm
- Weight gain and metabolic effects
- Consider prophylactic metformin; start at 500 mg for 1 week, then increase dose
- All patient should be referred for lifestyle management and exercise
- Myocarditis (rare; occurs only in the first 6 weeks of treatment)
- Baseline: check troponin I/T, CRP
- Obtain workup if patient reports chest pain
- Weekly troponin I/T and CRP for the first month
- Clozapine should be stopped if troponin ≥ 2x ULN or CRP > 100 mg/L
- Benign fever (~20%)
- In the absence of elevated troponin and myocarditis symptoms, fever is usually self-limited and there is no need to stop clozapine
- Seizures
- Valproate for myoclonic or generalized seizures
- Avoid phenytoin and carbamazepine because of kinetic interactions
- Pulmonary embolism (may include deep vein thrombosis or respiratory symptoms)
- Dilated cardiomyopathy
- Late complication; consider annual echocardiogram
- Increased risk of death and cerebrovascular events in elderly patients with dementia-related psychosis
Drug Interactions:
- Use clozapine plasma levels to guide treatment due to a propensity for drug interactions
- In presence of a strong CYP450 1A2 inhibitor (e.g., fluvoxamine, ciprofloxacin): use 1/3 the dose of clozapine
- In the presence of a strong CYP450 1A2 inducer (e.g., cigarette smoke), clozapine plasma levels are decreased
- May need to decrease clozapine dose by up to 50% during periods of extended smoking cessation (>1 week)
- Strong CYP450 2D6 inhibitors (e.g., bupropion, duloxetine, paroxetine, fluoxetine) can raise clozapine levels; dose adjustment may be necessary
- Strong CYP450 3A4 inhibitors (e.g., ketoconazole) can raise clozapine levels; dose adjustment may be necessary
- Clozapine may enhance the effects of antihypertensive drugs
Cardiac Impairment:
- Should be used with caution, particularly if the patient is taking concomitant antihypertensive or alpha 1 antagonist
Renal Impairment:
- Should be used with caution
Hepatic Impairment:
- Should be used with caution
Agomelatin = Valdoxan

1
AGOMELATINE
THERAPEUTICS
Brands • Valdoxan
see index for additional brand names
Generic? No
Class
• Neuroscience-based Nomenclature:
melatonin multi-modal (Mel-MM)
• Agonist at melatonergic 1 and melatonergic
2 receptors
• Antagonist at 5HT2C receptors
Commonly Prescribed for
(bold for FDA approved)
• Depression
How the Drug Works
• Actions at both melatonergic and 5HT2C
receptors may be synergistic and
increase norepinephrine and dopamine
neurotransmission in the prefrontal cortex;
may resynchronize circadian rhythms that
are disturbed in depression
• No influence on extracellular levels of
serotonin
How Long Until It Works
• Daytime functioning, anhedonia, and
sleep can improve from the first week of
treatment
• The onset of full therapeutic actions in
depression is usually not immediate, but
often delayed 2–4 weeks
• May continue to work for many years to
prevent relapse of symptoms
If It Works
• The goal of treatment is complete
remission of current symptoms as well as
prevention of future relapses
• Treatment most often reduces or even
eliminates symptoms, but not a cure since
symptoms can recur after medicine is
stopped
• Continue treatment until all symptoms are
gone (remission)
• Once symptoms gone, continue treating for
1 year for the first episode of depression
• For second and subsequent episodes of
depression, treatment may need to be
indefinite
If It Doesn’t Work
• Many patients have only a partial response
where some symptoms are improved but
others persist (especially insomnia, fatigue,
and problems concentrating)
• Other patients may be nonresponders,
sometimes called treatment-resistant or
treatment-refractory
• Consider increasing dose as early as
2 weeks after initiating treatment if
a response is insufficient (decision on dose
increase has to be balanced with a higher
risk of transaminase elevation; any dose
increase should be made on an individual
patient benefi t/risk basis and with strict
respect of liver function tests monitoring)
• Consider switching to another agent or
adding an appropriate augmenting agent
• Consider psychotherapy
• Consider evaluation for another diagnosis
or for a comorbid condition (e.g., medical
illness, substance abuse, etc.)
• Some patients may experience apparent
lack of consistent effi cacy due to activation
of latent or underlying bipolar disorder, and
require antidepressant discontinuation and
a switch to a mood stabilizer
Best Augmenting Combos
for Partial Response or
Treatment Resistance
• SSRIs (excluding fl uvoxamine), SNRIs,
bupropion, reboxetine, atomoxetine
(use combinations of antidepressant
with caution as this may activate bipolar
disorder and suicidal ideation)
• Modafi nil, especially for fatigue, sleepiness,
and lack of concentration
• Mood stabilizers or atypical antipsychotics
for bipolar depression, psychotic depression,
or treatment-resistant depression
• Benzodiazepines
Tests
• Liver function tests before initiation of
treatment and then after around 3 weeks,
6 weeks, 12 weeks, 24 weeks, and
thereafter when clinically indicated
• When increasing the dose, liver
function tests should be performed at
the same frequency as when initiating
treatment
• Liver function tests should be repeated
within 48 hours in any patient who
develops raised transaminases
Agomelatine.indd 1 gomelatine.indd 1 7/11/2017 4:05:56 PM /11/2017 4:05:56 PM
2
AGOMELATINE (continued)
augmentation strategies to treat side
effects
• Many side effects are time-dependent (i.e.,
they start immediately upon dosing and upon
each dose increase, but go away with time)
• Many side effects cannot be improved with
an augmenting agent
• Therotically activation and agitation may
represent the induction of a bipolar state,
especially a mixed dysphoric bipolar II
condition sometimes associated with
suicidal ideation, and require the addition
of lithium, a mood stabilizer or an atypical
antipsychotic, and/or discontinuation of
agomelatine (class warning)
SIDE EFFECTS
How Drug Causes Side Effects
• Adverse reactions usually mild to moderate
and occur within the fi rst 2 weeks of treatment
• Actions at melatonergic receptors and at
5HT2C receptors could contibute to the
side effects described below
Notable Side Effects
• Nausea and dizziness are most common
• Other adverse reactions are somnolence,
fatigue, insomnia, headache, anxiety,
diarrhea, constipation, upper abdominal
pain, vomiting, hyperhidrosis
• Increase of transaminase levels
Life-Threatening or
Dangerous Side Effects
✽ Rare hepatitis, hepatic failure
• Theoretically rare induction of mania (class
warning)
• Rare activation of suicidal ideation and
behavior (suicidality) (short-term studies
did not show an increase in the risk of
suicidality with antidepressants
compared to placebo beyond age 24)
(class warning)
Weight Gain
• Occurs in signifi cant minority
• Cases of weight decrease have been
reported
Sedation (Somnolence)
• Occurs in signifi cant minority
• Generally transient
• May be more likely to cause fatigue than
sedation
What to Do About Side Effects
• Wait
• Wait
• Stop if transaminase levels exceed 3 times
the upper limit of normal
• Switch to another drug
Best Augmenting Agents for Side
Effects
• Often best to try another antidepressant
monotherapy prior to resorting to
DOSING AND USE
Usual Dosage Range
• 25–50 mg/day at bedtime
Dosage Forms
• Tablet 25 mg
How to Dose
• Initial 25 mg/day at bedtime; after
2 weeks can increase to 50 mg/day
at bedtime
Dosing Tips
• If intolerable anxiety, insomnia, agitation,
akathisia, or activation occur either upon
dosing initiation or discontinuation,
consider the possibility of activated bipolar
disorder and switch to a mood stabilizer or
an atypical antipsychotic
Overdose
• Drowsiness and epigastralgia; fatigue,
agitation, anxiety, tension, dizziness,
cyanosis, or malaise have also been
reported
Long-Term Use
• Treatment up to 12 months has been found
to decrease rate of relapse
Habit Forming
• No
How to Stop
• No need to taper dose
Agomelatine.indd 2 gomelatine.indd 2 7/11/2017 4:05:56 PM /11/2017 4:05:56 PM
(continued) AGOMELATINE
3
Pharmacokinetics
• Half-life 1–2 hours
• Metabolized primarily by CYP450 1A2
Drug Interactions
• Use of agomelatine with potent CYP450
1A2 inhibitors (e.g., fl uvoxamine) is
contraindicated
• Tramadol increases the risk of seizures in
patients taking an antidepressant (class
warning)
Other Warnings/
Precautions
• Use with caution in patients with hepatic
injury risk factors, such as obesity/
overweight/non-alcoholic fatty liver disease,
diabetes, patients who drink large quantities
of alcohol and/or have alcohol use disorder,
or who take medication associated with risk
of hepatic injury. Doctors should ask their
patients if they have ever had liver problems.
• If symptoms or signs of potential liver
injury (dark urine, light-colored stools,
yellow skin/eyes, pain in upper right belly,
sustained new-onset and unexplained
fatigue) are present, agomelatine should be
discontinued immediately
• Use caution in patients with pre-treatment
elevated transaminases (> the upper limit
of the normal range and ≤ 3 times the
upper limit of the normal range)
• Discontinue treatment if serum
transaminases exceed 3 times the upper
limit of normal; liver function tests should
be performed regularly until serum
transaminases return to normal
• Agomelatine should be administered at
bedtime
• Use with caution in patients with bipolar
disorder unless treated with concomitant
mood-stabilizing agent
• When treating children off label (an
unapproved use), carefully weigh the
risks and benefi ts of pharmacological
treatment against the risks and benefi ts
of nontreatment with antidepressants and
make sure to document this in the patient’s
chart
• Warn patients and their caregivers about
the possibility of activating side effects
and advise them to report such symptoms
immediately
• Monitor patients for activation of suicidal
ideation, especially children and adolescents
Do Not Use
• If patient has hepatic impairment
• If patient has transaminase levels > 3 times
the upper limit of normal
• If patient is taking a potent CYP450 1A2
inhibitor (e.g., fl uvoxamine, ciprofl oxacin)
• If patient is taking an MAO inhibitor (MAOI)
• If patient has galactose intolerance, Lapp
lactase defi ciency, or glucose-galactose
malabsorption
• If there is a proven allergy to agomelatine
SPECIAL POPULATIONS
Renal Impairment
• Drug should be used with caution
Hepatic Impairment
• Contraindicated
Cardiac Impairment
• Dose adjustment not necessary
Elderly
• Effi cacy and safety have been established
(< 75 years old)
• Dose adjustment not necessary
• Should not be used in patients age
75 years and older
• Should not be used in elderly patients with
dementia
Children and Adolescents
• Carefully weigh the risks and benefi ts
of pharmacological treatment against
the risks and benefi ts of nontreatment
with antidepressants and make sure to
document this in the patient’s chart
• Monitor patients face-to-face regularly,
particularly during the fi rst several weeks
of treatment
• Safety and effi cacy have not been established
and it is not recommended
Pregnancy
• Controlled studies have not been
conducted in pregnant women
• Not generally recommended for use during
pregnancy, especially during fi rst trimester
Agomelatine.indd 3 gomelatine.indd 3 7/11/2017 4:05:58 PM /11/2017 4:05:58 PM
4
AGOMELATINE (continued)
Primary Target Symptoms
• Depressed mood, anhedonia
• Functioning
• Anxiety within depression
Pearls
• Agomelatine represents a novel approach to
depression through a novel pharmacologic
profi le, agonist at melatonergic MT1 /
MT2 receptors and antagonist at 5HT2C
receptors acting synergistically
• This synergy provides agomelatine with
a distinctive effi cacy profi le, different
from conventional antidepressants with
potentially an early and continuous
improvement over time
• Agomelatine improves anhedonia early in
treatment
• Improves anxiety in major depressive
disorder
• May be fewer withdrawals/discontinuations
for adverse events than with other
antidepressants
• No signifi cant effect on cardiac parameters
such as blood pressure and heart rate
• Some data suggest that agomelatine
may be specially effi cacious in achieving
functional remission
• Agomelatine may improve sleep quality
by promoting proper maintenance of
circadian rhythms underlying a normal
sleep-wake cycle
• Must weigh the risk of treatment (fi rst
trimester fetal development, third trimester
newborn delivery) to the child against
the risk of no treatment (recurrence
of depression, maternal health, infant
bonding) to the mother and child
• For many patients this may mean
continuing treatment during pregnancy
Breast Feeding
• Unknown if agomelatine is secreted in
human breast milk, but all psychotropics
assumed to be secreted in breast milk
• Therefore, breast feeding or drug needs to
be discontinued
• Immediate postpartum period is a high-risk
time for depression, especially in women
who have had prior depressive episodes,
so drug may need to be reinstituted late
in the third trimester or shortly after
childbirth to prevent a recurrence during
the postpartum period
THE ART OF PSYCHOPHARMACOLOGY
Potential Advantages
• Patients with lack of energy, anhedonia,
anxious comorbidity, and sleep-wake
disturbances
• Patients particularly concerned about
sexual side effects
Potential Disadvantages
• Patients with hepatic impairment
Agomelatine.indd 4 gomelatine.indd 4 7/11/2017 4:05:58 PM /11/2017 4:05:58 PM
(continued) AGOMELATINE
5
Suggested Reading
DeBodinat C , Guardiola-Lemaitre B , Mocaer
E , et al. Agomelatine, the fi rst melatonergic
antidepressant: discovery, characterization,
and development . Nat Rev Drug Discov
2010 ; 9 : 628 –42.
Goodwin GM , Emsley R , Rembry S , Rouillon F.
Agomelatine prevents relapse in patients with
major depressive disorder without evidence
of a discontinuation syndrome: a 24-week
randomized, double-blind, placebo-controlled
trial . J Clin Psychiatry 2009 ; 70 : 1128 –37.
Kennedy SH , Avedisova A , Belaïdi C ,
Picarel-Blanchot F , de Bodinat C . Sustained
effi cacy of agomelatine 10 mg, 25 mg, and
25–50 mg on depressive symptoms and
functional outcomes in patients with major
depressive disorder. A placebo-controlled
study over 6 months . Neuropsychopharmacol
2016 ; 26 (2): 378 –89.
Khoo AL, Zhou HJ, Teng M, et al. Network
meta-analysis and cost-effectiveness analysis
of new generation antidepressants. CNS Drugs
2015;29(8):695–712 .
Martinotti G , Sepede G , Gambi F , et al.
Agomelatine versus venlafaxine XR in the
treatment of anhedonia in major depressive
disorder: a pilot study . J Clin Psychopharmacol
2012 ; 32 (4): 487 –91.
Racagni G , Riva MA , Molteni R , et al. Mode
of action of agomelatine: synergy between
melatonergic and 5-HT2C receptors . World J
Biol Psychiatry 2011 ; 12 (8): 574 –87.
Stahl SM , Fava M , Trivedi M , et al. Agomelatine
in the treatment of major depressive disorder.
An 8 week, multicenter, randomized,
placebo-controlled trial . J Clin Psychiatry
2010 ; 71 (5): 616 –26.
Stahl SM . Mechanism of action of
agomelatine: a novel antidepressant exploiting
synergy between monoaminergic and
melatonergic properties . CNS Spectrums
2014 ; 19: 207 –12.
Stein DJ , Picarel-Blanchot F , Kennedy
SH. Effi cacy of the novel antidepressant
agomelatine on anxiety symptoms in
major depression . Hum Psychopharmacol
2013 ; 28 (2): 151 –9.
Taylor D , Sparshatt A , Varma S , Olofi njana O .
Antidepressant effi cacy of agomelatine: metaanalysis
of published and unpublished studies .
BMJ 2014 ; 348 : g2496.
Agomelatine.indd 5 gomelatine.indd 5 7/11/2017 4:05:58 PM /11/2017 4:05:58 PM
Agomelatine.indd 6 gomelatine.indd 6 7/11/2017 4:05:58 PM /11/2017 4:05:58 PM
Lurasidone : Latuda

What’s of Interest:
- Latuda is now approved for pediatric bipolar depression (ages 10 and older)
Brands
- Latuda
Class
- Atypical antipsychotic (serotonin-dopamine antagonist; second generation antipsychotic; also a mood stabilizer)
Approved For:
- Schizophrenia (ages 13 and older)
- Bipolar depression (ages 10 and older, monotherapy)
- Bipolar depression (adults, adjunct)
Formulation:
- Tablet 20 mg, 40 mg, 60 mg, 80 mg, 120 mg
How To Dose in Children and Adolescents:
- Schizophrenia: initial 40 mg once daily with food; maximum recommended dose 80 mg/day; often a good idea to initiate at 20 mg to test for tolerability before raising the dose to 40 mg, especially in children and in small body weight adolescents
- Bipolar depression: initial 20 mg once daily with food; can increase after 1 week; maximum recommended dose of 80 mg/day
Dosing Tips:

- Lurasidone should be taken with food (i.e., at least a small meal of a minimum of 350 calories)
- In children and adolescents, use lower starting dose for those without prior exposure to antipsychotics, especially if not switching from another antipsychotic
- In patients who have no prior exposure to antipsychotics, there may be more nausea than in those who have been exposed
- Studies in adults show side effects are less frequent when given at night than when given during the day
- Some children benefit from twice daily dosing mostly to improve tolerability
Weight Gain:
- Weight gain was not apparent in short-term adolescent studies
- In adult studies, many experienced about one- to two-pound weight gain greater than placebo in short-term 6-week trials; patients in long-term 52-week trials actually lost 1.5 pounds on average
- However, children and adolescents may be more susceptible to side effects
Sedation:
- Many patients experience and/or can be significant in amount
- May be higher in short-term trials than in long-term use
Other Notable or Dangerous Side Effects:
- Dose-dependent sedation, dizziness
- Akathisia, EPS (EPS, also called drug-induced parkinsonism)
- Nausea, vomiting
- Dose-dependent hyperprolactinemia
- May increase risk for diabetes and dyslipidemia
- Rare tardive dyskinesia (risk may be higher in children than it is in adults)
- Tachycardia, first-degree AV block
- Hyperglycemia, in some cases extreme and associated with ketoacidosis or hyperosmolar coma or death, has been reported in patients taking atypical antipsychotics
- Rare neuroleptic malignant syndrome (much reduced risk compared to conventional antipsychotics)
- Rare seizures
Warnings:
- Use with caution in patients with conditions that predispose to hypotension (dehydration, overheating)
- Dysphagia has been associated with antipsychotic use, and lurasidone should be used cautiously in patients at risk for aspiration pneumonia
- As with any antipsychotic, use with caution in patients with history of seizures
- Carefully weigh the risks and bene?ts of pharmacological treatment against the risks and bene?ts of nontreatment with an antipsychotic; it is a good idea to document this in the patient’s chart
- In children and adolescents, consider distributing brochures provided by the FDA and the drug companies
- When lurasidone is used to treat depressive episodes in children, it is a good idea to warn patients and their caregivers about the possibility of activating side effects and suicidality (as for any antidepressant in this age group) and advise them to report such symptoms immediately
Contraindications:
- If patient is taking a strong CYP 3A4 inhibitor (e.g., ketoconazole) or inducer (e.g., rifampin)
- In patients with a history of angioedema
- If there is a proven allergy to lurasidone
Pharmacokinetics:
- Half-life in adults is 18–31 hours (shorter half-life better documented at the 40 mg dose)
- In pediatric clinical trials (ages 10 to 17), the exposure of lurasidone was similar to that in adults, without adjusting for body weight
- Metabolized by CYP450 3A4
- Cmax and bioavailability are reduced if taken without food
Drug Interactions:
- Inhibitors of CYP450 3A4 (e.g., nefazodone, fluvoxamine, fluoxetine, ketoconazole) may increase plasma levels of lurasidone
- Coadministration of lurasidone with a strong CYP450 3A4 inhibitor (e.g., ketoconazole) or with a strong CYP450 3A4 inducer (e.g., rifampin) is contraindicated
- Coadministration of lurasidone with moderate CYP450 3A4 inhibitors can be considered; recommended starting dose is 20 mg/day; recommended maximum dose is 80 mg/day
- Moderate inducers of CYP450 3A4 may decrease plasma levels of lurasidone
- May increase effect of antihypertensive agents
- May antagonize levodopa, dopamine agonists
Pregnancy:
- Effective June 30, 2015, the US FDA requires changes to the content and format of pregnancy and lactation information in prescription drug labels, including the elimination of the pregnancy letter categories; the Pregnancy and Lactation Labeling Rule (PLLR or final rule) applies only to prescription drugs and will be phased in gradually for drugs approved on or after June 30, 2001
- Controlled studies have not been conducted in pregnant women
- Animal studies do not show adverse effects
- There is a risk of abnormal muscle movements and withdrawal symptoms in newborns whose mothers took an antipsychotic during the third trimester; symptoms may include agitation, abnormally increased or decreased muscle tone, tremor, sleepiness, severe difficulty breathing, and difficulty feeding
- Not teratogenic in rodents
- Psychotic symptoms may worsen during pregnancy and some form of treatment may be necessary
- National Pregnancy Registry for Atypical Antipsychotics: 1-866-961-2388 or http://womensmentalhealth.org/clinical-and-research-programs/pregnancyregistry
Renal Impairment:
- In adults, moderate and severe impairment: initial 20 mg/day; maximum dose 80 mg/day
- Possibly reduce these doses by half in children and adolescents
Hepatic Impairment:
- In adults, moderate impairment: initial 20 mg/day; maximum dose 80 mg/day
- In adults, severe impairment: initial 20 mg/day; maximum dose 40 mg/day
- Possibly reduce these doses by half in children and adolescents
Cardiac Impairment:
- Should be used with caution because of theoretical risk of orthostatic hypotension, although low potency at alpha 1 receptors suggests this risk may be less than for some other antipsychotics
- Lurasidone is one of the few antipsychtoics that does not have a warning for QTc prolongation
التحدي بآيات القرآن
في كل عصر من العصور سيظهر من يتقول على الرسول و يتطاول على القرآن
الكريم وورد التحدي بالقران الكريم في خمس آيات من خمس سور،
سميت آيات
التحدي هي على ترتيب السور
((وَإِنْ كُنتُمْ فِي رَيْبٍ مِمَّا نَزَّلْنَا عَلَى عَبْدِنَا فَأْتُوا بِسُورَةٍ مِنْ مِثْلِهِ وَادْعُوا شُهَدَاءَكُمْ”
مِنْ دُونِ اللَّهِ إِنْ كُنتُمْ صَادِقِينَ ” البقرة 23
أَمْ يَقُولُونَ افْتَرَاهُ قُلْ فَأْتُوا بِسُورَةٍ مِثْلِهِ وَادْعُوا مَنِ اسْتَطَعْتُمْ مِنْ دُونِ اللَّهِ إِنْ كُنْتُمْ”
صَادِقِينَ” [يونس 38
أَمْ يَقُولُونَ افْتَرَاهُ قُلْ فَأْتُوا بِعَشْرِ سُوَرٍ مِثْلِهِ مُفْتَرَيَاتٍ وَادْعُوا مَنِ اسْتَطَعْتُمْ مِنْ دُونِ اللَّهِ إِنْ كُنْتُمْ صَادِقِينَ” [هود: 13
قُلْ لَئِنْ اجْتَمَعَتْ الْإِنسُ وَالْجِنُّ عَلَى أَنْ يَأْتُوا بِمِثْلِ هَذَا الْقُرْآنِ لَا يَأْتُونَ بِمِثْلِهِ وَلَوْ كَانَ بَعْضُهُمْ لِبَعْضٍ ظهيرا ” الآية 88
“أَمْ يَقُولُونَ تَقَوَّلَهُ بَل لَّا يُؤْمِنُونَ * فَلْيَأْتُوا بِحَدِيثٍ مِّثْلِهِ إِن كَانُوا صَادِقِينَ”
الطور33-34
و هذا أبلغ رد عما يلمح به بعض ضيوف ومذيعين الفضائيات حاليا دون انفعال
ومكروا مكرا كبارا
لست أعرف بالتفصيل ماذا فعل قوم نوح حتى يشكو لربه و يقول “وَمَكَرُوا مَكْرًا كُبَّارًا (22)”
هل افتعلوا أزمات وقود وضوء و نعتوه بالتخلف ؟
هل استعانوا بأمثال تامر أمين وأديب ولميس وألأبراشي والغيطي وموسى ووظفوا لجان تضليل تطلق الشائعات والمشتتات لطمس الحق وتزيين الباطل؟؟
..هل دربوا شخص مثل افساد البحيري ولقبوه المفكر الاسلامي وصدروه المشهد ؟؟
..هل قاموا بكرنفال راقص من 6-9 مساءا على أضواء وألعاب الليزرو الآيس كريم و الترمس و اللب ..كتب السيناريو له الكذاب الأشر هيكل وهو طاعن في السن وأخرجها له المتاجر بأدب و صور الفراش والفقر و العشوائيات فاسد يوسف؟؟..ثم اسموها ثورة 30 يونيو و احتفلوا بذكراها ونسجوا حولها الخيالات وسبقوا الزمن في تدريسها للحاق جيل صغير يصدق كذبتهم؟

..هل ساقوا أي من أهله الى المعتقلات و السجون بدون محاكمات وأطلقوا أحكام اعدامات جماعية ؟
هل قاموا بتصفية جسدية لرجال في بيوتهم دون الافصاح عن أي ذنب اقترفوه؟
هل قاموا بقتل رجال فيهم أخوة لهم وقت السجود ثم كرموا القائمين على الذبح بأرقى المناصب و حصنوهم بأعلى القوانين؟
ربما فعلوا كل هذا و أكثر ولكن نوح عليه السلام لم يتوقف عن دعوتهم للحق و أعلن لهم وأسرر لهم و “ثُمَّ إِنِّي دَعَوْتُهُمْ جِهَارًا (8) ثُمَّ إِنِّي أَعْلَنتُ لَهُمْ وَأَسْرَرْتُ لَهُمْ إِسْرَارًا (9) ” ولكن هيهات …فدعا عليهم جهارا “وَقَالَ نُوحٌ رَّبِّ لَا تَذَرْ عَلَى الْأَرْضِ مِنَ الْكَافِرِينَ دَيَّارًا (26)
..منعوه من كل شئ و لكنهم لم يستطيعوا حرمانه حق الدعاء جهارا ..هناك قوم آخرون يحرمون حتى حق الدعاء
https://www.youtube.com/watch?v=3xba6mi2Flo
…اليوم الذكرى الخامسة لأحداث الحرس الجمهوري ..البعض يسميها مذبحة أو مجزرة ..
التحقيقات أسفرت اان المصلين ذبحوا بعضهم بعضا..كيف يستطيع المشاركين فيها النوم أو تناول الطعام أو تقلد المناصب ..
على صفحات الويكيبديا القصة بأكثر من رواية أقلهم ان استشهد 65 شهيد في أقل من ساعة و لا قصاص حتى الآن ..” قُل رَّبِّ إِمَّا تُرِيَنِّي مَا يُوعَدُونَ (93) رَبِّ فَلَا تَجْعَلْنِي فِي الْقَوْمِ الظَّالِمِينَ (94)” المؤمنون
https://ar.wikipedia.org/wiki/%D8%A3%D8%AD%D8%AF%D8%A7%D8%AB_%D8%A7%D9%84%D8%AD%D8%B1%D8%B3_%D8%A7%D9%84%D8%AC%D9%85%D9%87%D9%88%D8%B1%D9%8A
أرق مريض و الاختفاء القسري
لم تكن حالات الاختفاء القسري و التي تزيد عن الف بعد ثورة يونيو المجيدة هي الاولى في التاريخ ، فقد سجل لنا القرآن قبل ذلك بكثير حالة تفهم حينها انها كذلك ، فقد اختفى اصحاب الكهف و الرقيم من المدينة و آوو الى كهفهم هربا من سفه المدينة و ملتها و ظلم أهلها ، و لك ان تتخيل كم دفع أهل هؤلاء الفتية من رشاوي في أقسام الشرطة و سعوا الى وساطات للمحافظ و الحاكم و الوالي للافراج عن اولادهم المختفين ظنا منهم انهم في أحد المعتقلات، و لم يخطر ببالهم انهم نائمين في احد الكهوف، و المدهش هو استهلال القصة ف الآية ٩ من سورة الكهف

“أَمْ حَسِبْتَ أَنَّ أَصْحَابَ الْكَهْفِ وَالرَّقِيمِ كَانُوا مِنْ آيَاتِنَا عَجَبًا”
أي هل تظن ان ذلك كان بالعجيب أو المدهش أو نادر الحدوث ، هل يحتمل معنى هذه الآيه ان هذه القصة قابلة للتكرار ،
اضطرت ذات مرة لقول ذلك لأب يشكو من أرق مزمن لثلاث سنوات متصلة ولم تفلح معه كل وصفات الأدوية العديدة في يده و حينما سألته هل يرتبط أرقه بحدث في حياته فقال منذ اختفاء ابني ضاع نومي، و قال لي ساقوه للمعتقل اول مره دون اي ذنب يقترفه و كذلك في المرة الثانية اما في الثالثة فاختفى ولم يعد وذنبه الوحيد انني أنا أبوه و أرادوا تعذيبي به،
خلعت هذه الكلمات أحشائي ، فاستعنت بهذا التفسير ربما كان نائما ، أليس النوم نعمة كبيرة في هذا العصر ، لو كان هناك حبة او دواء تجعلك تنام مئة عام و تستيقظ لتسأل ماذا حل بأديب و لميس وبقري و الغيطي و كل الأفاقين المنافقين المدلسين والكذابين! ، ماذا حل بالمحصنيين أنفسهم بالقوانين؟و المحيطين ذاتهم بحرسهم!؟ و قواتهم ومواكبهم!! ، ما اخبار المستخفين بعقول الناس ؟و المستهزئين بآيات الله؟ ، الام انتهى السلام الرائع الدافئ مع اسرائيل؟ اليست نعمة كبيرة ان تنام هذه الأيام و السنين ، اعتبر ولدك نائما في احد الكهوف و اكتب قصته حتى يعلمها احفاد أحفادك و حينما يستيقظ يعرفونه
الغريب انني وجدت لمحة الفرح و الانشراح على وجه الأب و كتبت له علاج بسيط للنوم و انقطعت أخباره و قابلته بالصدفة بعد عام و سألته عن الأرق كيف أصبح فقال
لي الحمدلله طبيعي ، فسألت هل بسبب الدواء. فقال لا أقنعت نفسي ان ولدي نائم و سيستيقظ يوما ما!
“(9) إِذْ أَوَى الْفِتْيَةُ إِلَى الْكَهْفِ فَقَالُوا رَبَّنَا آَتِنَا مِنْ لَدُنْكَ رَحْمَةً وَهَيِّئْ لَنَا مِنْ أَمْرِنَا رَشَدًا (10) فَضَرَبْنَا عَلَى آَذَانِهِمْ فِي الْكَهْفِ سِنِينَ عَدَدًا (11) ثُمَّ بَعَثْنَاهُمْ لِنَعْلَمَ أَيُّ الْحِزْبَيْنِ أَحْصَى لِمَا لَبِثُوا أَمَدًا (12) نَحْنُ نَقُصُّ عَلَيْكَ نَبَأَهُمْ بِالْحَقِّ إِنَّهُمْ فِتْيَةٌ آَمَنُوا بِرَبِّهِمْ وَزِدْنَاهُمْ هُدًى (13) وَرَبَطْنَا عَلَى قُلُوبِهِمْ إِذْ قَامُوا فَقَالُوا رَبُّنَا رَبُّ السَّمَاوَاتِ وَالْأَرْضِ لَنْ نَدْعُوَ مِنْ دُونِهِ إِلَهًا لَقَدْ قُلْنَا إِذًا شَطَطًا (14) هَؤُلَاءِ قَوْمُنَا اتَّخَذُوا مِنْ دُونِهِ آَلِهَةً لَوْلَا يَأْتُونَ عَلَيْهِمْ بِسُلْطَانٍ بَيِّنٍ فَمَنْ أَظْلَمُ مِمَّنِ افْتَرَى عَلَى اللَّهِ كَذِبًا (15) وَإِذِ اعْتَزَلْتُمُوهُمْ وَمَا يَعْبُدُونَ إِلَّا اللَّهَ فَأْوُوا إِلَى الْكَهْفِ يَنْشُرْ لَكُمْ رَبُّكُمْ مِنْ رَحْمَتِهِ وَيُهَيِّئْ لَكُمْ مِنْ أَمْرِكُمْ مِرفَقًا (16) وَتَرَى الشَّمْسَ إِذَا طَلَعَتْ تَزَاوَرُ عَنْ كَهْفِهِمْ ذَاتَ الْيَمِينِ وَإِذَا غَرَبَتْ تَقْرِضُهُمْ ذَاتَ الشِّمَالِ وَهُمْ فِي فَجْوَةٍ مِنْهُ ذَلِكَ مِنْ آَيَاتِ اللَّهِ مَنْ يَهْدِ اللَّهُ فَهُوَ الْمُهْتَدِ وَمَنْ يُضْلِلْ فَلَنْ تَجِدَ لَهُ وَلِيًّا مُرْشِدًا (17) وَتَحْسَبُهُمْ أَيْقَاظًا وَهُمْ رُقُودٌ وَنُقَلِّبُهُمْ ذَاتَ الْيَمِينِ وَذَاتَ الشِّمَالِ وَكَلْبُهُمْ بَاسِطٌ ذِرَاعَيْهِ بِالْوَصِيدِ لَوِ اطَّلَعْتَ عَلَيْهِمْ لَوَلَّيْتَ مِنْهُمْ فِرَارًا وَلَمُلِئْتَ مِنْهُمْ رُعْبًا (18) وَكَذَلِكَ بَعَثْنَاهُمْ لِيَتَسَاءَلُوا بَيْنَهُمْ قَالَ قَائِلٌ مِنْهُمْ كَمْ لَبِثْتُمْ قَالُوا لَبِثْنَا يَوْمًا أَوْ بَعْضَ يَوْمٍ قَالُوا رَبُّكُمْ أَعْلَمُ بِمَا لَبِثْتُمْ فَابْعَثُوا أَحَدَكُمْ بِوَرِقِكُمْ هَذِهِ إِلَى الْمَدِينَةِ فَلْيَنْظُرْ أَيُّهَا أَزْكَى طَعَامًا فَلْيَأْتِكُمْ بِرِزْقٍ مِنْهُ وَلْيَتَلَطَّفْ وَلَا يُشْعِرَنَّ بِكُمْ أَحَدًا (19) إِنَّهُمْ إِنْ يَظْهَرُوا عَلَيْكُمْ يَرْجُمُوكُمْ أَوْ يُعِيدُوكُمْ فِي مِلَّتِهِمْ وَلَنْ تُفْلِحُوا إِذًا أَبَدًا (20) وَكَذَلِكَ أَعْثَرْنَا عَلَيْهِمْ لِيَعْلَمُوا أَنَّ وَعْدَ اللَّهِ حَقٌّ وَأَنَّ السَّاعَةَ لَا رَيْبَ فِيهَا إِذْ يَتَنَازَعُونَ بَيْنَهُمْ أَمْرَهُمْ فَقَالُوا ابْنُوا عَلَيْهِمْ بُنْيَانًا رَبُّهُمْ أَعْلَمُ بِهِمْ قَالَ الَّذِينَ غَلَبُوا عَلَى أَمْرِهِمْ لَنَتَّخِذَنَّ عَلَيْهِمْ مَسْجِدًا (21) سَيَقُولُونَ ثَلَاثَةٌ رَابِعُهُمْ كَلْبُهُمْ وَيَقُولُونَ خَمْسَةٌ سَادِسُهُمْ كَلْبُهُمْ رَجْمًا بِالْغَيْبِ وَيَقُولُونَ سَبْعَةٌ وَثَامِنُهُمْ كَلْبُهُمْ قُلْ رَبِّي أَعْلَمُ بِعِدَّتِهِمْ مَا يَعْلَمُهُمْ إِلَّا قَلِيلٌ فَلَا تُمَارِ فِيهِمْ إِلَّا مِرَاءً ظَاهِرًا وَلَا تَسْتَفْتِ فِيهِمْ مِنْهُمْ أَحَدًا (22) وَلَا تَقُولَنَّ لِشَيْءٍ إِنِّي فَاعِلٌ ذَلِكَ غَدًا (23) إِلَّا أَنْ يَشَاءَ اللَّهُ وَاذْكُرْ رَبَّكَ إِذَا نَسِيتَ وَقُلْ عَسَى أَنْ يَهْدِيَنِ رَبِّي لِأَقْرَبَ مِنْ هَذَا رَشَدًا (24) وَلَبِثُوا فِي كَهْفِهِمْ ثَلَاثَ مِئَةٍ سِنِينَ وَازْدَادُوا تِسْعًا (25) قُلِ اللَّهُ أَعْلَمُ بِمَا لَبِثُوا لَهُ غَيْبُ السَّمَاوَاتِ وَالْأَرْضِ أَبْصِرْ بِهِ وَأَسْمِعْ ما لَهُمْ مِنْ دُونِهِ مِنْ وَلِيٍّ وَلَا يُشْرِكُ فِي حُكْمِهِ أَحَدًا (26)”
Psychiatry’s ‘C’ words
Recently, contemporary “culture” has capriciously confounded and confused our national community with a cringe-worthy “C” word. Unfortunately, this was followed by only transient public consternation, reflecting the coarsening of our social communication and discourse and the cant of many. But the ripple effects continue.
As a psychiatrist who closely observes the human condition, I contemplated the current confrontational tone in the media and wondered how corrosive language can confuse and cloud our sensibilities.
Then it occurred to me that there are many commendable clinical “C” words that describe what we psychiatrists do in daily practice. We stay calm while facing crises, and help our patients achieve certainty when stress makes them confused. We compassionately comfort and care for our suffering patients. We strive to engender courage and confidence when fragile patients are confronted with continuous criticism by callous and condescending people. We remain composed when we counsel patients with confrontational and crabby moods and help correct their confusing conflicts. We coordinate their care with courtesy, always aspiring for a cure for their corroded emotional condition.
But then I felt compelled to go further and call on my creativity to consider “C” words that describe severe psychiatric clinical disorders. I came up with the following cogent cascade of common characteristics of serious mental disorders:
- Cerebral pathology
- Circuit disruptions of neural connections
- Chemical imbalance
- Cytokine inflammatory conflagration
- Cognitive impairment
- Chronic course
- Crippled functioning.
My compulsion continued. I decided to contemplate more “C” words that capture our therapeutic course of action to correct a patient whose cortico-limbic circuitry is being threatened with considerable, even calamitous collapse. My consideration led to clarity, and I came up with the following list of what we psychiatrists conform to in our clinical practice:
- Connect with patients
- Correct diagnosis
- Course-specific intervention
- Choose the appropriate medication
- Combine cognitive-behavioral therapy with medication
- Cognitive assessment at baseline
- Compliance/concordance with treatment
- Continuity of care
- Comorbidities, physical and psychiatric
- Collaborative care with other medical specialists
- Comprehensive treatment plan with other mental health professionals.
A book about dirty words written by a psychoanalyst called the “C” expletive the worst of all cuss words.1 Its recent emergence in the national media compromised our civility and created a cesspool of contemptible conversations. Let’s transcend the contemptible “C” word of a caustic contemporary “culture” (which had its 15 minutes of infamy), and consider the many coherent and congenial “C” words of psychiatric practice that bring peace of mind and contentment to those who suffer from psychiatric brain conditions. As for the compulsive or involuntary use of curse words that begin with a “C,” or any other letter, psychiatry has a clinical term for it: coprolalia.
New marijuana-based pharmaceutical drug approved by FDA

What is Epidiolex?
Epidiolex is an oral liquid-based drug made from the cannabidiol (CBD) portion of cannabis. Compared to the tetrahydrocannabinol (THC) portion, CBD is not psychoactive, so taking this drug would not result in a high for the user.
CBD acts on different parts of the nervous system compared with THC. According to the Centers for Disease and Control (CDC), THC and CBD both may be useful for nausea caused by cancer treatments. Neither marijuana-derived substances, however, have been medically approved since they both fall under the Schedule 1 drug classification, which refers to substances that are usually illegal, often abused and have no proven medical benefit, according to the Drug Enforcement Administration.

Why was it approved?
The drug was approved by the FDA on Monday after a review of four large studies that looked at Epidiolex for the treatment of Lennox-Gastaut syndrome and Dravet syndrome in both adults and children.
The first major study looked at the effect of Epidiolex for Lennox-Gastaut syndrome was also published in The New England Journal of Medicine in May. In the study, the researchers enrolled 225 patients, ages 2 to 55 (all of whom had two or more seizures per day) to two different doses of Epidiolex or a placebo that contained no medicine. The trial lasted 14 weeks. The average seizure frequency dropped by 41.9 percent in the higher dose group and by 37.2 percent in the lower dose group and was down 17.2 percent in the placebo group (an inactive placebo often has a medicinal effect).
It is known as the potential for CBD in seizure treatment for years, and it is expected a response.
The second major study was published in The New England Journal of Medicine in May, and it looked at the effect of Epidiolex for Dravet syndrome. Researchers enrolled 120 children and young adults to compare Epidiolex to standard anti-epileptic treatment. After 14 weeks, the average seizure frequency dropped by at least half in 43 percent of people who took Epidiolex and 5 percent of the people taking the medication became seizure-free.
Both Dravet Syndrome and Lennox-Gastaut syndrome are diagnosed by a clinical exam and EEG by a doctor, ideally a doctor who specializes in brain conditions for children, known as a pediatric neurologist. Dravet Syndrome is confirmed with a genetic test.
What are the side effects of this medication?
In the trial, the main side effect was liver toxicity, which appeared as increased liver enzymes.
Others may have felt more sedated, nauseous or experienced diarrhea or vomiting, but these were not life-limiting symptoms.
There is some research that indicates that CBD specifically could interact with other medications such as statins, and increases the amount of those medications in the blood.