
Long-Acting Injectable Antipsychotics:
Who should receive LAIs?
Consider LAIs for patients with recent-onset schizophrenia and those with risk factors for medication nonadherence:
history of non-adherence, severe symptoms, comorbid substance use, cognitive impairment,
ambivalence or negative attitudes towards medications, and poor insight.
Are the newer LAIs more effective?
The effectiveness of newer LAIs (aripiprazole, olanzapine, paliperidone and risperidone) and older LAIs
(haloperidol,fluphenazine, flupenthixol) is similar.
Practical considerations
Abilify Mantenna
Aripiprazole monohydrate requires a period of overlap of 2 weeks with oral aripiprazole.
Available as a lyophilized powder which needs to be reconstituted.
Aristada
Aripiprazole lauroxil requires a period of overlap of 3 weeks with oral aripiprazole.
Available as a prefilled syringe that does not require reconstitution.
Zyprexa Relprevv
Olanzapine pamoate does not need overlap with oral olanzapine.
It has a small risk of post-injection syndrome (0.07% of injections):
o Symptoms include sedation, confusion, agitation, anxiety, aggressiveness, dizziness, ataxia and
extrapyramidal symptoms
o This risk limits use olanzapine pamoate use
o After injection, the patient must be monitored for three hours by a healthcare professional
o In the US, prescribers who administer Zyprexa Relprevv must enroll in a national registry that
documents the incidence of this adverse effect
Invega Sustenna
Paliperidone palmitate does not need overlap with oral paliperidone.
Requires two separate loading dose injections during the first week.
Invega Trinza
The 3-month paliperidone palmitate (PPM–3) formulation can only be used if the patient has been receiving 1-
month paliperidone palmitate injections for at least 4 months.
It is administered 4 times a year, providing the longest interval of any approved LAI.
Risperdal Consta
Risperidone microspheres requires a period of overlap of 3 weeks with oral risperidone.
It has a 2-week dosing interval.
Anxiety
Lower your Cholesterol without medication
You can begin to reduce your “bad” LDL cholesterol by making a few simple changes in your diet.
If your cholesterol is creeping upward, your doctor has probably told you that diet and exercise — the traditional cornerstones of heart health — could help to bring it down. And if you’d prefer to make just one change at a time, you might want to begin with your diet. A major 2012 analysis of several controlled trials involving hundreds of men and women found that dietary changes reduced LDL and total cholesterol while exercise alone had no effect on either. (However, adding aerobic exercise did enhance the lipid-lowering effects of a heart-healthy diet.)
The people in the studies followed a variety of diets, from Mediterranean to low-fat to low-calorie. However, the most effective diets substituted foods with cholesterol-lowering power for those that boost cholesterol. While you may have to say goodbye to a few snacks and fast foods, you can replace them with others that are equally satisfying. “You don’t have to follow an all-or-nothing approach. It’s really a matter of common sense,” she says. She suggests a few ways to start getting your cholesterol under control.
Weed out the worst fats
There is so much evidence implicating trans fats in heart disease that the FDA has proposed removing the “generally recognized as safe” designation from them. “The first thing we do when I’m counseling patients is to go over all the sources of trans fats in their diet and make substitutions,” ..
Trans fats are created by adding hydrogen to a liquid fat to help it solidify. Food manufacturers started using trans fats because they extend the shelf life of packaged baked goods. Fast-food purveyors took to them because they can be reused again and again. Although public pressure has forced the food industry to phase out trans fats, they haven’t disappeared entirely. To avoid eating them inadvertently, scrutinize the labels on food packages before you put them in your shopping cart. If you see “partially hydrogenated” in the list of ingredients, pass that product by. If trans fats aren’t banned from restaurants in your area, ask if the cook uses partially hydrogenated oil before you order.
Saturated fats and dietary cholesterol, which are derived primarily from animal products, aren’t exactly heart-healthy, but it’s all right to eat them in small amounts. Because eggs are such a good source of nutrients, it’s okay to have as many as four yolks a week and whites as often as you like. Yes to red meat, shrimp, lobster, high-fat cheeses, butter and organ meats — but only to small portions of each one every couple of weeks or so.
Eat more of the better fats
Both polyunsaturated and monounsaturated fatty acids help lower LDL. Most plant-derived oils, including canola, safflower, sunflower, olive, grapeseed, and peanut oils, contain both. Fatty fish (such as salmon, tuna, trout, herring, and mackerel), seeds, nuts, avocados and soybeans are also great sources.
Go crazy with color
Fruits and vegetables have scads of ingredients that lower cholesterol — including fiber, cholesterol-blocking molecules called sterols and stanols, and eye-appealing pigments. The heart-healthy list spans the color spectrum — leafy greens, yellow squashes, carrots, tomatoes, strawberries, plums, blueberries. As a rule, the richer the hue, the better the food is for you.
Don’t be too refined
Whole grains are another good source of fiber. Instead of refined flour and white rice, try whole-wheat flour and brown or wild rice. Old-fashioned oatmeal is also a good choice, but not the quick-cooking versions, which have had much of the fiber processed out.
And don’t substitute sugar for fat. “It’s one of the worst choices you can make,” McManus warns. Food manufacturers may boost the sugar content of low-fat salad dressings and sauces to add flavor. If you see sugar, corn syrup, or any word ending in “ose” near the top of the list of ingredients, choose a higher-fat version without trans fats instead.
Remember: Calories still count
All fats, whether good or bad, have nine calories per gram — about 100 calories a tablespoon. While you switch to a heart-healthy diet you may need to keep tabs on your calorie intake for a while.
Your Core in office work
One of the best things you can do for your health is to strengthen your core muscles.
Your core is more than just abdominal muscles; it includes the muscles in your back, sides, pelvis, and butt. They’re the muscles that allow you to reach, bend, and move freely.
What’s more, a strong core helps keep you steady on your feet. And that’s critical because it can help you stay independent by preventing debilitating falls.
How is your balance? Take this 10-second balance test right now:
Stand comfortably near a wall with your arms in any position you choose. Lift one foot an inch or two off the floor so that you are balancing on the other foot. If you can’t hold this position for more than 10 seconds, you’re at risk for a fall. See page 16 of Gentle Core Exercises for ways to increase your core strength and improve your balance.

The office workout
The following routine is a great way to ease into core work. You can do these four exercises at work, without your colleagues being any the wiser. You can do these exercises at home, too, thanks to simple variations. The front plank, for example, can be done while either leaning on your desk or using the kitchen counter to support your weight.

Equipment needed: Desk (a table or countertop is also fine), exercise mat, and sturdy chair.

Time can pass awfully slow when you’re hoping to see results after embarking on a new exercise regimen. But if you do gentle core work consistently, you can start to see progress in as little as two to four weeks. Once you do, you might wonder when and how to progress from there or how to just maintain the gains you’ve made. Either way, our tips below will help.
When to progress

Repeatedly challenging muscles makes them stronger. As you get stronger, exercises in your routine will become easier to do. You’re ready to progress if you can manage all four of these tasks throughout each exercise:
- maintain good form
- stick to the specified tempo
- use a full, or comfortable, range of motion
- complete the suggested number of reps or hold the position for the suggested number of seconds.
How to progress
You can continue to challenge your muscles by making one of these choices:
- adding sets (up to two, if specified in the instructions)
- trying the higher level variation of the exercise
- moving up to a more challenging core regimen.

How to maintain gains
At some point, you may be satisfied with the gains you’ve made. To maintain gains, continue your routine, sticking to the highest level of challenge you’ve achieved.
If you get sick or take time off for other reasons, you may need to drop down a level or do fewer reps and sets before building up again.
What if you begin to feel bored? Go over your goals again. Then vary your core work by trying a new workout or selecting new exercises to do throughout the day.
Write Your CV Simple

Find more education infographics on e-Learning Infographics
YOUR WORKING OFFICE AND YOUR POSTURE!
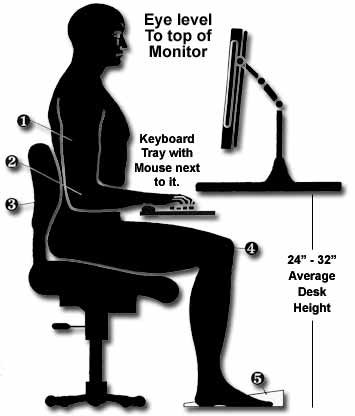
Did you know you can dramatically improve your keyboarding output if you only slightly improve your office ergonomics and posture?
Posture can affect how quickly and even how accurately you touch type, and using the principles of ergonomics to give your posture a few tweaks can enable you to touch type in a way that increases your productivity while decreasing risk to your health.
Be Aware of Bad Posture
People with office-bound jobs need to be aware of back pain and any other physical pain caused in their hands, their feet, and in their neck and back. A poorly-designed office chair, a too-short desk, or a badly lit screen that forces you to hunch over your desk are all possible causes of body pain.
Being aware of your posture when working, walking, and standing will ensure you always sit upright and avoid posture that affects your health and compromises your touch typing efficiency.
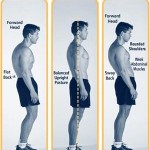
Get to Know Your Ergonomics

Whether sitting in a chair at the office or standing waiting for your coffee at the counter, your body has to be aligned. Take a moment to visualize yourself sitting at your office chair. Starting at your head and going to the bottom of your spine, you should see a straight vertical line.
If you’re hunching your shoulders or leaning to one side, then your posture is disturbed, which will increase the chances of triggering back, wrist, and shoulder pain.
To IMPROVE POSTURE consider adopting these health-promoting, ergonomic habits:
– Don’t sit for prolonged periods of time. Move around at regular intervals.
– Avoid sitting with your legs crossed.
– Don’t lean to one side or lean on your arm when sitting.
– Remove direct light that is causing glare on your computer screen.
– Ensure your monitor is at eye level. Use books or other props to put the screen higher, or a pillow to make yourself taller.
– Sit in ergonomically-designed office chairs and use props that support good posture and take the pressure off of your spine and back.
– Try sitting on a balance ball; it’s another way to ensure better posture.
– Give footrests a try as well – they can take some of the strain off of your back when sitting for long periods of time. They’re also helpful if your feet don’t reach the floor.
– Keep your arms open at a 90 degrees angle, and make sure your feet are in that position also. Extending your arms in front of you, or crossing your feet underneath you, disrupts the alignment of your spine.
Get Regular Exercise
Exercise keeps your body strong and your muscles fit. This can alleviate back pain, and any other pain caused due to prolonged sitting, or sitting in the wrong position.
Restorative exercise can also help you improve your posture. Physical activities that boost your core strength and balance include yoga and pilates.
Overall, choose an active lifestyle to ensure your body and muscles are healthy and strong, and that you minimize the health hazards associated with sitting. This not only will ensure you’re healthy, but will also help you make the most of your typing efficiency
للتوحد قصة منسية

منذ ما يقرب 50 سنة و على وجه التحديد في عام 1943 .. كان هناك طبيب أطفال أمريكي نابه اسمه ليو كانر يعمل في مستشفى جونز هوبكينز كتب مقال يصف 11 حالة لأطفال مرضى يعيشون مع أنفسهم في عالم خاص بهم على حد تعبيره – لا يتعاملوا حتى مع أهلهم
يشعرون بالفزع لأقل شئ و يصرخوا و لا يتواصلوا مع أحد بأي صورة ولا شكل
الأمهات لايشعرن أن لديهم أبناء ويبكون على حال أطفالهم
كانر قال ان هذه الحالات نادرة جدا و أن كل مجموع الحالات التي رآها في حياته الطبية 11 حالة فقط
لكن في عام 1950 غير ما قاله و زعم انها ليست نادرة كما كان يظن و ان بلغ عدد الحالات التي رآها أكثر من 150 طفل و انه لم يكن يعطي أهمية للحالات بشكل مناسب
يا ترى لماذا زعم في البداية انها حالات نادرة و بعدها زاد التشخيص ..!!؟؟ ذلك لأن المعايير التي وضعها هو للتشخيصكانت منتقاه جدا و دقيقي للغاية .يعني مثلا كان لا يقبل التشخيص بالتوحد لأي طفل عنده صرع سواء كان تشنجي أو غير تشنجي لأنه قد تكون سبب حالته النوبات الصرعية
كانر كان فخور بانه رفض 9 حالات من أصل عشر حالات تم تويلها اليه من أطباء زملاء و أطباء نفسيين على أساس انه لازم تشمل المعايير التي حددها هو
كان مصمم انه يصل بأن التوحد نوع من أنواع فصام الأطفال ناجمة عن قساوة الآباء أو جمودهم و برودهم العاطفي على حد تعبيره FRozen Parents و عشان كده أولادهم يكونوا بارديين و جامديين عاطفيا

و قال الأطفال في حالة تجمد غير قابل للذوبان
أيضا هو لاحظ ان بعض هؤلاء الأطفال لهم قدرات خاصة في الحساب – الموسيقى قوة الذاكرة حتى انه وصف طفل عنده بالعيادة في عمر سنتين فقط استطاع التمييز بين أكثر من 30 سيمفونية ولما كانت أمه تشغل السيمفونية ينطق بشكل صحيح اسم السيمفونية و يقول بيتهوفن أو باخ أو غيره و يقوم بعمل ترانيم تتماشى مع السيمفونية بشكل متقن جدا

من معايير كانر ان الأطفال لا يستطيعوا تمييز الخطر و يجروا بلا هدف بشكل أهوج و مندفع ويصرخون بلا مشاعر و بالطبع كان وصفه لهؤلاء الأطفال و الآباء وصمة عال لكل من في بيته توحد و مصدر خجل كبير لهم و بالتالي بدءوا يدخلوا المصحات و ينفصلوا عن أهلهم
استمرت هذه المعلومات و دخلت مناهج كلية الطب و الطب النفسي حتى سنة 1970 وكل الأطباء اللي كتبوا عن التوحد كانوا متأثرين بكلام كانر و علمه ورؤيته و زادوا في الوصف شويه لكن كانت معايير كانر صعبة للغاية و لا تزال تجزم بأن الحالات شديدة الندرة

في لندن كان في لورا ونج ..كانت معالجة نفسية و كانت هي و زوجها حنونيين جدا و كانت مؤمنة بنظرية كانر في التوحد
و كان عنها طفلة اسمها سوزي
لورا كانت عارفة صعوبة تربية طفلة كثل سوزي بدون دار رعاية و لا أدوات خاصة و لا مدارس أهلية
وصلت طلباتها للجهات المسؤولة و قررت تدرس مدى انتشار المرض و عدم اعتباره نادر الحدوث حتى تهتم الجهات الحكومية المسؤولة
قالوا لها اعملي دراسة و لو طلع مرض مش نادر و موجود هنوفر دعم مالي و نبدأ أبحاث عليه


بحثوا عن كل الحالات الممكنة فأدركوا وقتها ان معايير كانر في التشخيص محدودة جدا و في معايير أكثر مما ذكر و أوضح يجب أن نأخذها في الاعتبار كان في أطفال لا تتكلم نهائي و أطفال لا تتوقف عن الكلام باسهاب في الفلك في البيولوجي في الحيوانات لكن كلام غير مرتب و منظم و يصح أجزاء منه لو عاد ترتيبه
حاولوا يبحثوا عن أي بحوث .. كانت قليلة جدا لكن و جدوا بحث وحيد باللغة الألمانية و لم يترجم و نشر سنة 1944 يعني سنة واحدة بعد كانر

كاننشره باحث ألماني اسمه هيومان أسبرجر .. لكن مفيش حد خد باله منه خالص و لا يفتكر البحث و لا مترجم ..كان كان عرف البحث لكن لم تترجم له بالكامل
أسبرجر كان بيدير مدرسة في فيينا من سنة 1930 و كان مهتم بالاطفال اللي عندهم صعوبات التعلم و كان بيستعمل الموسيقى في التعليم و يبدأ بها الحصة و ينظم مسرحيات كل أسبوع
أسبرجر لم يلم الأهل بالبرود و الجمود العاطف
حاول أسبرجر انه لن يتعامل مع الأطفال كمرضى في عيادته بل كان بيلقبهم اساتذتي الخاصصينspecial professoers
اعتبر التوحد نطاق و طيف كبير بين الاعاقة و الموهبة و قال ان صفات التوحد شائعة بين العامة و الخاصة
وقال ان طرق التواصل مع الأطفال المتوحديين مختلفة زي عالم شارد الذهن أو مخترع متشتت أو باحث اجتماعي مبهدل في ملابسه
بل أكثر من كده

اعتبر انك عشان تكون ناجح في نوع من الفن أو الرياضيات لازم يكون عندك قدر من طيف التوحد و قال ان كلام كانر عن الآباء كله غلط
و لم يتفق مع معايير كانر ووأوسع المعايير فهما و شمولية
ترجمت لورا بحث اسبرجر و غيرت مفاهيم كانر
وبعدين ظهر علينا فيلم ي و لم يقل انهم هم اللي جابوا المرض لابنهم بل على العكس كان مدرك انه بيتعامل مع مرض محتاج لتجهيزات كثيرة ووسائل راحة مدى الحياة
رجل المطر و المبدع داستن هوفمان كيف بدل مشاعر أخوه المادية الى مشاعر عاطفية و ترك كل الارث لأخيه
لماذا ..ليه ابني أنا اللي جاله المرض؟
لا ينظر بالعين
لا يبدأ بحوا و لا يحافظ عليه
لا يبتسم ولا يضحك بشكل اجتماعي طبيعي
يصرخ عند الضغط عليه
كلماته محدودة و أغليها مبهم
لم يستطع التعلم و المدرسة
طبيب الأطفال و النفسية و الأعصاب لم يفيدونا بالشكل المناسب
لماذ
.. يمكن التطعيمات .. يمكن تطعيم الحصبة .. كان في حالات في أمريكا أعلنوا عنها و بعدين رجعوا فيها..التطعيمات و المصل و اللقاح برئ من التوحد
أطباء الوراثة بيقولوا طبيعي .. مفيش وراثة و لا بحث واحد يؤكد عنصر الوراثة .. لكن لقينا أكثر من حالة في الاسرة الواحدة .. طيب لو كان عندي أب له 4 أطفال توحد من 3 زوجات ..هل يكون عنصر التوريث من الأب .. ربما >>أكثر من 300 جين وراثي تم عزلهم يمكن يكونوا مسؤولين عن التوحد ..دراسات بالغة التعقيد و العينة تتكلف أكثر من 5000 دولار وممكن تتعاد اكثر من مرة
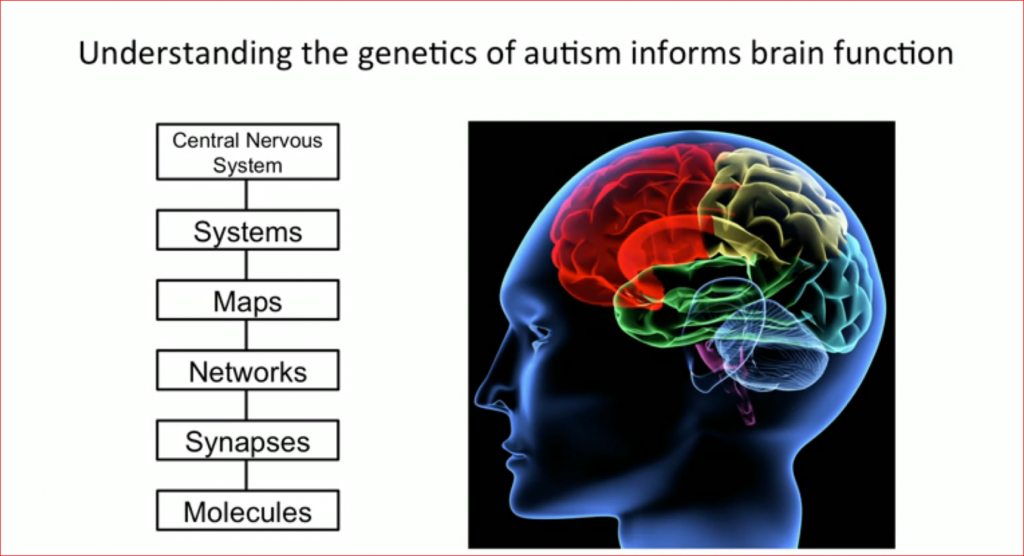
ممكن يكون بيولوجي .. نصورهم و هم بيتواصلوا بعينهم و نطور الدراسة .. واحد من العلامات المهمة جدا اللي تبدأ من الشهر الثاني و أحيانا من الأول ..الانتباه .. هز سلسلة المفاتيح لابنك ينتبه ليها و مررها شمال و بعدين يمين يروح لها.. الشئ البسيط ده لا يتكون عند أطفال التوحد
تعالى معايا لمخلوقات بدائية لو انت قرد و نظرت لقرد أكبر منك أو فصيلة أكبر منك ستخاف و تهرب ..لانه معناه انه قد يفتك بك
لو انت طير و نظر أحد في عينك تلف رأسك و تنظر بعيد فورا و تفزع و تهرب و تطير و لو في قفص تصرخ
Dementia Patient : To drive or not To drive!
Caring for a person with dementia or Alzheimer’s disease presents a range of challenges. Spouses, family members, and friends must deal with feelings of loss as the person they know seems to slip away. Supporting a loved one with basic activities of daily living can be time consuming and exhausting. And it is difficult to balance protecting the person you’re caring for and preserving what independence remains.
One of the trickiest problems for caregivers to negotiate with people with dementia is driving. The consequences of a misstep behind the wheel can be deadly.
Decisions about driving
Whether or not it is safe to drive can be complicated, particularly when the person is only mildly impaired. Some believe that driving privileges should not be taken away until a person is clearly an unsafe driver.
But can you identify an unsafe driver before an accident occurs?
Driving requires amazing coordination — the eyes, brain, and muscles must process information and respond to it quickly. Driving skills may seem sufficient until an unexpected situation occurs when a person with dementia can panic or freeze with indecision.
One way to gauge the risk is to observe the person’s general behavior. If friends and family see their loved one exhibit poor judgment, inattentiveness to what’s going on around him or her, clumsiness, and slow or inappropriate reactions, then that person should not get behind the wheel.
Taking away the keys

Ideally, a tactful and respectful approach will preserve the person’s self-esteem while getting them off the road. Some people may agree to stop driving for other reasons — for instance, the car needs repair or the license or registration has expired. You can also opt for a road test with a driver’s rehabilitation specialist, who can offer an independent assessment of safety. People with Alzheimer’s disease sometimes take seriously a written prescription from a physician that says, “Do not drive.”
In some states, doctors have a legal duty to report unsafe drivers and drivers with certain medical problems to the state department of motor vehicles. If all else fails, you may need to seek advice from a lawyer or an official with the Department of Public Safety in your state. Procedures vary, but generally a driver’s license can be suspended on the basis of a physician’s written statement.
My child’s Mobile
Did you know that 42% of US children ages 0 to 8 have their own mobile device?
Essentially all homes had a mobile device, up from half in 2011. Ninety-five percent of homes had a smartphone, 78% had a tablet, and, as I said before, 42% of children had their own mobile device. What’s interesting is that the 42% number was the same whether families were high- or low-income. Parents are buying mobile devices for their children, plain and simple.
The amount of time that young children spend in front of screens hasn’t changed much since 2011. On average, it’s about two hours a day (ranging from 42 minutes a day for the under-2 crowd to about three hours for the 5-to-8-year-olds). What has changed, though, is that kids 2 to 8 are spending about an hour a day on a mobile device.
In 2011, just six short years ago, kids under 8 spent about five minutes a day on mobile devices.
This explosion of mobile device use in children isn’t surprising, given the explosion of mobile device use overall. It’s also not necessarily bad. Two-thirds of parents in the survey thought that mobile device use helped their children learn, and they are right that there are lots of great ways mobile devices can do just that. Mobile devices can give children access to educational websites, apps, and videos — and things like Google Earth that can teach them about the world.
If that’s all kids did, this would all be good news. But that’s not all they do. Mostly, according to the report, they watch TV and play games on the devices. And 19% use them in restaurants, and 14% use them while eating meals, cutting into conversations they might have had with family and friends.
Also, they spend more time on mobile devices than reading, if they read at all. Only a little more than half of children 0 to 8 read or are read to — and only for an average of 30 minutes. While mobile devices can be used for reading, that’s not what kids are using them for.
That’s the thing: any device is only as good as what we use it for
When the use of any technology spreads and advances so quickly, it’s hard to be really thoughtful and careful about the implications. It’s perfectly natural to think of these devices as fun new toys — because they are. It’s perfectly natural, too, to think of them as full of potential — because they are. Our task as parents, caregivers, and educators is to be sure that the potential for our children is for good, not harm.
Here are some ways we can do just that:
- Make sure that the content children access with mobile devices is age-appropriate.
- Make the most of the time children spend on tablets and mobile devices. Look for educational games and videos, or applications that encourage creativity.
- Mobile devices will never be as good as interactions with other people, or hands-on experiences when it comes to learning and development. Make sure children get plenty of those, too. And make sure that mobile devices don’t get in the way of exercise or getting outdoors, both of which are important for children.
- While it’s tempting to use mobile devices as babysitters or something to amuse your child while you multitask, keep that to a minimum. Instead, do things together with them. Play games together. Watch a video together. Learn a language together. Have the mobile device bring you together rather than splitting you apart. Speaking of which…
- Have device-free zones and times. Like the dinner table or family time, or when friends are over (unless they are sharing a game together). The bedroom should be another one of those places. Make sure devices are off (and preferably charged elsewhere) at least an hour before bedtime, as the blue light they emit can make it hard to fall asleep.
- Talk with your children about mobile device use, especially social media use. Help them learn to be good digital citizens.
Activity trackers: Can they really help you get fit?

Lately, I’ve been checking the number of steps I take each day. It’s not hard to do. My phone tracks it without me even asking it to. It also tracks the number of flights of stairs I’ve climbed and the number of miles I covered. And there are other options: I could track how often I stand up, how many calories I’ve burned by being active, and how many minutes I’ve engaged in a brisk activity.
Even my employer has gotten into the act. As is common in many workplaces, one of our hospital’s wellness programs has organized “walking clubs” with teams comparing and competing with each other based on the number of steps team members take each week. Some companies offer prizes, financial incentives, or reductions in health insurance premiums if an employee participates in such a program.
Why all this monitoring?
The technology we carry around with us — our phones, watches, or other gadgets — allows enormous amounts of data to be collected about us every day. It’s important to keep in mind that there is a purpose to all of this. The point of activity trackers is to become more aware of how much (or how little) activity we’re doing so that we can make positive changes. Since the health benefits of physical activity — and the health risks of being sedentary — are well established, increasing activity is a health priority (or should be) for millions of people. Activity trackers are the first, um, step (sorry, couldn’t resist).
Do activity trackers really improve health?
My guess is that most people take for granted that activity trackers are helpful in promoting more physical activity, but that’s based mostly on assumption. That’s why researchers at Duke-National University of Singapore Medical School a designed Study to compare full-time employees who used activity trackers with those who did not. Each of the 800 employees enrolled in the study paid the equivalent of $7 to enroll and then were randomly assigned to one of four groups for one year:
- use of a Fitbit Zip, a popular clip-on activity tracker (with payment of $3/week to continue in the study regardless of the number of steps taken)
- a Fitbit plus a cash incentive ($11 for taking 50,000 to 70,000 steps each week, or $22 for more than 70,000 steps/week)
- a Fitbit plus a payment to a charity (which was larger with increased activity)
- a control group that did not use an activity tracker; this group also received the $3/week for participation regardless of activity levels.
Researchers monitored more than just the number of steps taken. Study participants also had to monitor of more vigorous exercise and physical activity, weight, blood pressure, fitness levels, and they were asked about the quality of life as well.
So, what did they find?
First, the good news
The group receiving the cash incentive increased their daily steps compared to the start of the study. This group was more active than the control group at six months, and 88% of them were still using their Fitbits (compared with about 60% of the Fitbit only and charity incentive groups).
Say it isn’t so!
When incentives stopped, only one in 10 study subjects continued to use the Fitbit. And after a year, with incentives stopped, activity levels fell in the groups receiving an incentive compared to when they started. This is disappointing indeed, especially considering that the participants in this study were probably more motivated than most to focus on their activity levels. They went to the effort and expense of enrolling in the study and agreed to put up with all the monitoring. In addition, most people in the real world probably have no direct financial incentives to maintain a certain level of activity each week.
This study follows another one from the University of Pittsburgh that found less weight loss among young adults who used fitness trackers compared to those who didn’t.
What’s next?
As technology evolves and research provides more information about what works (and what doesn’t), I think we’ll see a new generation of devices that are more customized to individual needs and medical conditions. For example, a person with diabetes might monitor physical activity to provide information about how to coordinate insulin injections and meals.
In addition, activity trackers can do more than simply spit out information about how active you’ve been. A good example comes from another recent study in which activity trackers were incorporated into a competitive game, complete with signed commitments to specific activity goals, an elaborate point system, and reliance on team cooperation and rewards. The study found that those using game-based activity trackers were more active and achieved activity goals more often than those using activity trackers without the game. The study lasted only 12 weeks and improvements waned somewhat after it ended, so the long-term impact of such a program is uncertain.
Physical activity trackers have quickly become a multimillion-dollar product category. I don’t see them going away anytime soon. But, to actually get people moving and have a positive impact on health, we’ll probably need to use them in more innovative ways. And if they claim to improve your health, we’ll need high-quality research to back that up.
Speed Reading : again and againg
What Is Speed Reading?
Speed reading is the process of rapidly recognizing and absorbing phrases or sentences on a page all at once, rather than identifying individual words.
The amount of information that we process seems to be growing by the day, whether it’s emails, reports, and websites at work, or social media, books, and magazines at home. We likely feel pressure to get this information more quickly.
Most people read at an average rate of 250 words per minute (wpm), though some are naturally quicker than others. But, the ability to speed read could mean that you double this rate.
We’ll now explore some of the skills that you can use to accelerate your reading.
How to Speed Read
All speed reading techniques have one thing in common: you avoid pronouncing and “hearing” each word in your head as you read it, a process known as for as “sub-vocalization.” Instead, you “skim” lines or groups of words, as you can understand words more quickly than you can say them.
One way to stop yourself from sub-vocalizing is to focus on blocks of words rather than on individual ones. Do this by relaxing your face and “softening” or expanding your gaze on the page, so that you stop seeing words as single, distinct units. As you practice this, your eyes will skip faster across the page.
Then, when you approach the end of a line, allow your peripheral vision to take your eye to the final set of words. This will help to stop pauses in your reading (often at full points), meaning that you scan across and down to the next line more quickly.
Now let’s look at three methods to boost your reading speed:
1. The Pointer Method
Utah school teacher Evelyn Nielsen Wood was one of the pioneers of speed reading. In the 1950s, she claimed that she could read at up to 2,700 wpm if she swept a finger along the line as she read.
This became known as the Pointer method, and is also sometimes called “hand pacing” or “meta guiding.” Holding a card under each line and drawing it down the page as you read works just as well.
2. The Tracker-and-Pacer Method
This is a variant of the Pointer method where you hold a pen, with its cap still on, and underline or track each line as you read it, keeping your eye on the tip of the pen. This will help to increase the pace at which you take in each line, and improve your focus on the words. Whether you actually underline the words is your choice.
Try to spend no more than one second on each line and then increase your speed with each subsequent page. You will probably find that you retain very little information at first, but, as you train your brain and you become more comfortable with the technique, your comprehension should improve.
Note:
An advantage of the Pointer and Tracker-and-Pacer methods is that they should reduce your need to skip back and re-read sentences – a hindrance to speed reading that is known as “regression.”
3. The Scanning (or Previewing) Method
“Scanning” involves moving your eyes quickly down the page – often down the center – and identifying specific words and phrases as you go. These can be key sentences (often the first sentence of each paragraph), names, numbers, or trigger words and ideas. Learning to expand your peripheral vision can help with this.
You won’t read every word, but your eye will land on what is important to allow you to grasp the basic idea. It may be helpful to use a mind mapping to organize the information you take in.
When to Speed Read
These techniques can all help you to read more quickly, but are they appropriate for what you’re trying to achieve?
Effective speed reading is a balance between pace and comprehension. Studies have found that the faster you read, the less information you take in, particularly when it comes to remembering the detail.
So, speed reading is clearly not the answer if you’re reading a complex legal or technical document, even if you are pushed for time. Similarly, it would be sensible to slow down if the material you’re reading is new or unfamiliar, or if you have to teach it to someone else.
When you need to understand only the basic arguments or conclusions being presented, though, using a speed reading technique can work.
This may especially be the case if you intend to go back and re-read something more slowly when you’re less busy. In fact, One study has suggested that skimming a text can improve your comprehension second time around.
Generally speaking, if you want to memorize something, you’ll need to read slowly, at less than 100 wpm. A normal rate for learning is 100-200 wpm, and for comprehension, it is 200-400 wpm.
Speed reading is normally done at a rate of around 400-700 wpm. Anything above 500-600 wpm means sacrificing comprehension, although this varies from person to person.
How to Improve Your Speed Reading
Knowing the “how” and “when” of speed reading is only the first step to success. Here are some more tips to help you:
- Avoid distractions. Create an environment where there are as few interruptions and distractions as possible, to allow you to focus fully on the words in front of you.
- Go easy. Read an uncomplicated novel or a simple online article to get a feel for which technique is going to work best for you. Gauge how much you’ve remembered or understood, and set a timer to see how much faster you are now reading.
- Cover words that you’ve already read. This helps you to stop your eyes flitting back to earlier words and slowing down your reading.
- Know what you want from the text. This can be useful if you are using the skimming method, as it primes you to pay attention when you see relevant words, sentences or phrases. You can then slow down at these points, or circle them for emphasis, but otherwise move across the page quickly.
- Benchmark your progress. This way you can tell whether your practice is paying off. There are many free speed reading assessments online, such as at ReadingSoft.com.
- Practice, practice, practice. You have to practice speed reading to get good at it. The more you train yourself, the more natural it will feel.
Know that
There are different techniques that you can use to improve your reading speed. All of them involve skimming a page rather than “sub-vocalizing” each word as you were likely taught at school.
Excellent speed reading involves practice and retraining yourself, as well as learning to focus more on what is in front of you and avoiding distractions.
But it is important to strike the right balance between speed and comprehension: sometimes speed reading is not appropriate or helpful.
Sex and Aging

Attitudes about sexuality and aging
Fantasies can help rev up your sex life. Myths, on the other hand, can stop desire dead in its tracks. Such myths aren’t the legends from classical history. They’re the stories we tell ourselves and each other to support the notion that older people shouldn’t, can’t, and wouldn’t want to have sex. This type of myth, however, bears as little relationship to reality as do the fanciful sagas of ancient gods and goddesses. Here are some examples of the most popular sexual myths and the myth-busting truths.
1. The myth: Only the young are sexually attractive.
The culture we live in exalts youth. Turn on the TV or open a magazine and you’ll be barraged with images of supple skin, firm flesh, and lustrous locks. But if your mirror is reflecting a different picture these days, you may feel like the party is going on without you.
The reality: Older can be quite sexy.
Sure, thinning hair, laugh lines, and a paunchy midriff are no picnic. But think back on what it was that made you attractive in your younger years. Was it your soulful brown eyes, your crooked smile, or maybe your infectious laugh? Chances are, those attributes are still as appealing as ever. In fact, a 1999 survey conducted by the AARP and Modern Maturity magazine revealed that the percentage of people age 45 and older who consider their partners physically attractive increases with age.
2. The myth: Sexuality in later life is undignified.
Whether it’s the white-haired grandmother fussing with her knitting or the loveable old codger puffing on a pipe, society is inclined to desexualize older adults. When older adults do express their sexuality, it’s often viewed with derision — for example, the stereotype of the “dirty old man.”
The reality: It’s healthy for older adults to express their sexuality.
People are living longer and remaining healthier. And they are more vigorous than ever before. Former president George H.W. Bush went skydiving to celebrate his 75th birthday, John Glenn returned to space at age 77, and Carol Sing forged a new world record at 57 by becoming the oldest woman to swim the English Channel. With this trend toward later-life vitality, why shouldn’t seniors be allowed to cast off outdated and ill-fitting stereotypes in order to express their normal, healthy sexual appetites?
3. The myth: Men and women lose their ability to perform sexually after a certain age.
Vaginal dryness and erectile difficulties loom large as you hurtle past 50. You may be feeling that you should just listen to what your body is trying to tell you: Sex is a thing of the past.
The reality: You can still have a satisfying sex life.
While a certain degree of physical change is unavoidable, this fact of life doesn’t necessarily translate into insurmountable sexual problems. For men, the Viagra revolution means most erection problems can be corrected with little medical intervention. For women, high-tech vaginal lubricants and hormone creams and rings are viable substitutes for what nature no longer supplies. What’s important for both sexes to remember, though, is that a softer erection, reduced natural lubrication, or a less intense orgasm doesn’t mean you’re no longer interested in your partner or in sex itself. For many couples, these kinds of changes provide an impetus for developing a new, rich, and satisfying style of lovemaking — one that’s based more on extended foreplay and less on intercourse and orgasm.
4. The myth: Sex is boring when you get older.
Drooping libido, slower rates of arousal, and the predictability of having the same partner for 20 or more years all add up to a ho-hum sex life.
The reality: Sex is as good as you make it.
While it’s true that a 19-year-old will have a faster, harder erection and a more forceful ejaculation than his 55-year-old counterpart, it doesn’t mean the quality of the experience is necessarily better. On the contrary, the older man has better control of his ejaculations. Less penile sensitivity means he may be able to enjoy a wider range of erotic sensations and maintain his erection longer. And his experience may pay off in improved sexual technique and a better understanding of what will please his partner.
Many women begin to find sexual confidence in their 30s, and this blossoms with maturity. As a woman moves through her 40s, her orgasms actually become more intense, and she can still have multiple orgasms. After menopause, when she’s free of any worry about pregnancy, she can give herself over to the pure enjoyment of sex.
Although longtime partners do have to contend with issues of familiarity in their relationship, these problems can be offset by greater emotional intimacy and trust. Because inhibitions often lessen with age, sex at 50 or 60 may include a level of experimentation and playfulness you wouldn’t have dreamed of in your younger years.
By the numbers: Statistics on sexuality and sexual satisfactionIn 1999, Modern Maturity magazine and the AARP foundation polled 1,384 adults age 45 and older about the role sex played in their lives. The findings paint a detailed picture of sexuality at midlife and later. The importance of sex Over all, the majority of men (66.8%) and women (56.7%) responding felt that a satisfying sex life was important to their quality of life. But an even higher percentage (91.9% of men and 87.1% of women) thought that a good relationship with their spouse or partner played a key role in their happiness. Frequency of sexual activity Of individuals with partners, just over 60% in the youngest age bracket surveyed (45–59) had intercourse at least once a week. At age 75, the proportion dropped to one in four. Still, nearly three-quarters of respondents of all ages had intercourse once a month or more, provided they had partners. However, when the group was examined as a whole, one out of five men and two out of five women had not participated in any form of sexual touching or caressing over the last six months. Men tended to think about sex and feel sexual desire more frequently than women. While rates of intercourse were similar for both sexes, more men than women reported engaging in sexual touching. Self-s timulation on a regular basis was also about eight times higher among men. Factors affecting sexual satisfaction Not surprisingly, one of the major factors associated with respondents’ satisfaction was the availability of a partner. In the 45–59 age group, roughly four out of five individuals had partners; by comparison, only one in five women over 75 had partners. Declining health also appeared to have an effect on sexual activity and satisfaction. On a list of features that might improve their sexual satisfaction, the men ranked better health for themselves or their partners at the top. Although impotence emerged as a significant issue for nearly a quarter of the men, less than half of those men had ever sought medical treatment for the problem. |
||
Table 3. Survey facts and figures |
||
| What participants said, in a nutshell | Men | Women |
| A good relationship with a spouse or partner is important to quality of life | 91.9% | 87.1% |
| My partner is physically attractive | 59% | 52.9% |
| A satisfying sexual relationship is important to my overall quality of life | 66.8% | 56.7% |
| Sexual activity is a pleasurable but not a necessary part of a good relationship | 50.4% | 52.9% |
| Had sexual intercourse at least once a week during the last six months | 43% | 35% |
| Engaged in kissing or hugging at least once a week during the last six months | 74% | 48% |
| Am satisfied with my sex life | 54.9% | 54% |
| Better health for myself would improve my sex life | 30.3% | 15.9% |
| Better health for my partner would improve my sex life | 22.1% | 19.4% |
| Have taken medication to improve sexual functioning | 10% | 7% |
| Sex becomes less important to people as they age | 38.7% | 36.5% |
Emotional and social issues
“The brain is the body’s most important sex organ.” This oft-repeated phrase bears more than a little truth. While the initial prerequisites for sexual activity are physiological — functional sex organs, adequate hormone levels, and freedom from healt h conditions that interfere with the body’s ability to respond to erotic cues — these elements don’t guarantee sexual satisfaction. Stress, anxiety, self-esteem issues, negative past experiences, lifestyle demands, loss of loved ones, and relationship conflicts can weigh heavily. During midlife and beyond, these factors, combined with naturally occurring physical changes, can make you vulnerable to sexual problems.
Lack of a partner
It may seem obvious that not having a partner is an impediment to an active sex life, but it’s an especially important issue for older people. By age 65, many people find themselves alone, through either divorce or widowhood. This affects sexuality in a variety of ways.
According to the AARP/Modern Maturity Sexuality Survey, 64% of men with partners and 68% of women with partners are primarily satisfied with their sex lives. This is in sharp contrast to the small proportion of those without partners (18% of men and 28% of women) who are pleased with their sex lives.
The partner gap is a particular problem for American women because their average life span (79 years) is more than five years longer than that of men. Because American women marry men who are on average three years older, that can mean even more time alone. Should a woman want to remarry, her chance of finding a new mate in her age bracket dwindles yearly; there is an average of only 7 men for every 10 women age 65 and above. All this boils down to the fact that, compared with men, women are likely to live a greater portion of their lives without a mate.
Finally, starting a new sexual relationship after divorce or the death of a spouse can present its own dilemmas. People often fear that they will not become aroused or be able to have an orgasm with a different partner. They also may be self-conscious about baring their body in front of someone new. Because a new relationship may come along months or years after their last sexual relationship, some individuals feel anxious that they have “forgotten how to have sex” or that “the equipment doesn’t work anymore.” For those who have lost a much-loved spouse, feelings of guilt or disloyalty at starting a new relationship can be overwhelming.
Relationship issues
Tension in a relationship can be deadly to a couple’s sex life. In many cases, conflict is at the root of a sexual problem. Other times, a sexual issue strains a couple’s ability to get along. The following issues are often connected to sexual problems.
Anger and frustration. Accumulated anger, hurt, disappointment, and resentment can fester, destroying closeness between partners. These pent-up feelings often extinguish the flames of desire. For men, anger and frustration can interfere with arousal and getting an erection. Likewise, the breakdown of trust can be devastating to a woman’s ability to reach orgasm. Both partners can suffer loss of libido in a conflict-ridden environment. This type of disappointment turns toxic when one or both partners resort to criticism and defensiveness — two of the major harbingers of divorce. In addition, one member of the couple may unconsciously withhold sex as a way of expressing anger or to maintain the upper hand in a situation where he or she feels otherwise powerless.
Poor communication. Communication is essential for partners to build the trust needed for a successful sexual relationship. By talking frankly about your feelings, you can foster acceptance and understanding in your relationship. This makes it easier for you and your partner to collaborate on finding solutions to issues, and it can prevent resentments from piling up. When conversation breaks down, anger and resentment are likely to build.
Dialogue is especially vital as physical changes take place. Vaginal dryness or erection difficulties can be wrongly perceived as waning interest in sex, which can trigger feelings of rejection and resentment. By articulating feelings, couples can sort out the physiological factors from the emotional and relationship issues, and address each appropriately.
Boredom. Once the honeymoon is over, almost every couple has to contend with boredom sooner or later. The person who was once so electrifyingly mysterious to you may become as comfortable — and as alluring — as an old shoe. While the deep trust and intimacy created from years of shared experiences are the building blocks of a truly loving relationship, such familiarity can take the edge off desire. Sex may not even seem worth the trouble when you’re facing the same old lovemaking routines.
When sexual activity wanes, other types of physical affection often fade, too. This lack of physical connection can extend the emotional distance between you and your partner. As a result, it’s all the more difficult to resume sexual intimacy later on. But it’s possible to do so.
One frequent motivator for a person to have an affair is a quest for newness. This yearning may arise from a need to banish midlife drudgery, a desire to find out what sex is like with someone else, or an urge to recapture the heart-pounding sexual highs of youth. Other times, an individual searches out a new partner to meet unfulfilled emotional or intellectual needs. An affair sometimes occurs because of sexual dysfunction in the marriage. For example, men who have erection difficulties or women who can’t reach orgasm may seek out new lovers to prove that the sexual problem is their spouse’s doing, not their own. Likewise, the partners of those with sexual difficulties may try to seek reassurance that they’re still sexually appealing in the arms of someone else.
Affairs. While researchers can’t seem to agree on how many people seek sex outside their marriage — the estimates range from 20% to 60% — one thing is clear: An affair is often an indication of an unmet need in the relationship.
The reverberations of an affair can extend throughout a couple’s relationship like ripples on a pond. Sometimes the straying partner isn’t able to respond sexually to his or her spouse because of guilt over the affair, fatigue from juggling two sexual relationships, or a negative comparison of the spouse with the new lover. If the spouse discovers the affair, he or she may withdraw emotionally.
An affair can be a serious, sometimes fatal, blow to a relationship. However, it’s possible for a marriage not only to survive infidelity, but also to grow from this painful expe rience. To do this, though, both partners must face the personal and relationship issues that led to the affair in the first place. Couples therapy is a good place to turn for help in doing this. Sex therapy can also be useful if the affair has caused or resulted from sexual problems.
The Viagra revolution
In the years since the famous “little blue pill” entered the market in March 1999, millions of couples have seen firsthand what this drug can and can’t do. In many cases, Viagra (sildenafil citrate) is the answer to a prayer for men who have been unable to have an erection. But the drug offers no help in untangling the emotional and relationship pressures that frequently accompany erectile dysfunction.
For one thing, Viagra only works if there is desire to have sex. If emotional issues are impinging on libido, the pill won’t help. It’s important that the partner of a man who has begun taking Viagra understands this. During a long bout with erectile dysfunction, many women blame themselves for their partner’s inability to perform. When Viagra comes onto the scene, the woman may find it hard to let go of past feelings of rejection. She may mistakenly assume that her husband’s newfound erections are merely a chemical phenomenon, not an outgrowth of sexual attraction to her.
When intercourse is suddenly a possibility again, relationship issues can sprout up or resurface. For example, dramatic differences in libido sometimes emerge. Also, a woman can develop problems related to vaginal atrophy if she hasn’t had sex in a long time. She may need to undergo a few weeks of therapy using medication or dilators before she can comfortably resume intercourse.
The bottom line is that couples should try to regard Viagra as an opportunity to become erotic again, while realizing that it is neither a mandate to have intercourse nor a panacea for every problem in the bedroom.
Performance anxiety
Defined as an overwhelming concern about sexual performance that obscures pleasure and leads to sexual dysfunction, performance anxiety is a particularly insidious issue affecting aging couples. Performance anxiety becomes a particular problem for men as they move into their 50s. It’s the most common psychological contributor to erectile dysfunction.
Here’s how the problem often develops. The natural effects of aging dictate that a man needs more time and direct penile stimulation for an erection. Medications and cardiovascular disease may also contribute to erection difficulties. If a man continues to expect the instantaneous rock-hard erections of his 20s, he may equate this change in his physical response with the end of his virility. Once he makes this erroneous leap, the problem snowballs. After a few incidences of erection failure, embarrassment and feelings of defeat leave him unwilling to try again. He may withdraw from all forms of intimacy to avoid having to perform. In turn, his partner feels rejected and fears that she’s no longer attractive enough to sexually excite him. She may also suspect him of having an affair.
If this happens, the woman may shy away from touching her partner sexually out of fear that another failure will occur. Paradoxically, her reticence denies the man just the type of direct stimulation that he needs at this stage of life to achieve an erection. The result is that an addressable physical issue becomes a morass of anger, resentment, and frustration.
Women, too, can experience performance anxiety. Frank discussion of sexuality has become commonplace in women’s magazines and on daytime television. This openness has had the unintended consequence of making some women worry that they do not respond quickly or intensely enough to be considered a “good lover.”
At one point or another, you may have come to the realization that gravity is not kind to your body as you age. Nor is childbirth, a fatty diet, lack of exercise, or the hormone declines that lead to muscle loss, loose skin, and thinning hair. But what does this have to do with your sex life? It can have everything to do with it if you let it. Worry about having your partner see your sagging breasts or potbelly can discourage you from even thinking about having sex. If you do decide to be intimate, you may demand that sex take place only under the covers, with the lights out, while you’re wearing a T-shirt. Needless to say, these conditions don’t leave much room for inspired lovemaking. You may also find that your preoccupation with your appearance while making love prevents you from fully enjoying sex.
Body image and self-esteem
Relationship conflicts can ensue. When one partner needs constant reassurance about his or her attractiveness and becomes overly sensitive to perceived criticism, it can foster mutual resentment. The paradox in this dynamic is that the majority of middle-aged and older adults responding to the AARP/Modern Maturity Sexuality Survey said they still found their partners physically or romantically attractive. What’s more, the percentage increased with age.
By shifting your focus away from your perceived flaws to your attributes — for example, your eyes or your hair — you can boost your self-esteem and establish your own standards for attractiveness. Also, try directing your attention to the experience of giving and receiving pleasure during sex. This can help you find the confidence to give yourself over to the experience. Great sex is often the outgrowth of a deep emotional connection — something that’s not guaranteed by having a perfect body.
A negative self-image isn’t always rooted in your appearance. Career setbacks or other disappointments can lead to feelings of failure and depression, both of which sap desire. For men, episodes of impotence can undercut confidence in their manhood. No matter what its cause, a poor self-image can take a toll on your sex life. When performance anxiety develops as a result, it can spark a downward spiral of repeated sexual failure and diminishing self-esteem. Correcting this problem demands serious attention to its origin. Because feelings of low self-worth are a symptom of depression, you should talk to a doctor if the problem persists.
Your sexuality is a natural drive that’s with you from birth, but your family and cultural background shape your attitudes toward sex. As you become an adult, your own experiences further influence your sexuality. The result for many is a healthy enjoyment of sex, but others may have more mixed feelings. The changes that take place in midlife and beyond often exacerbate issues about sex. Deeply entrenched negative associations can also emerge during this time.
Expectations and past experiences
For example, women (and men) — particularly those who came of age before the so-called sexual revolution in the ’60s — may cling to the notion that it is improper for “nice girls” to enjoy sex. This belief can be damaging for both partners. A woman who has merely acquiesced to sex as a duty to her husband or as a necessary step in childbearing may feel uncomfortable seeking sexual pleasure. Her partner may interpret this lack of enthusiasm as a reflection of her feelings about him.
Inexperience and embarrassment over discussing sexual matters may hamper people from fully expressing themselves sexually. For example, intercourse alone does not give many women the kind of stimulation they need for fulfilling sex, and uneasiness about discussing the problem prevents some couples from developing techniques that could offer the woman greater pleasure. Compounding the problem, childhood taboos against masturbation may prevent a woman from ever discovering the means to her sexual pleasure, so she’s unable to direct her partner in this regard. It may be more comfortable for a woman to forgo her own pleasure than to confront these matters. She may ultimately resort to faking orgasms rather than risk asking for a different approach to lovemaking. When this pattern exists for years, revealing the truth would mean admitting to a longstanding deception, which could shake the trust in the relationship and injure her partner’s self-esteem.
Alternately, a man may feel his self-worth depends on his ability to please his partner. His focus during sex, therefore, is on performing rather than succumbing to pleasure. If his partner doesn’t immediately respond to his efforts, feelings of inadequacy can pervade the relationship, eroding the couple’s bond. This dynamic can ultimately lead to performance anxiety and related sexual problems.
During the early years of a couple’s relationship, such missed connections are often masked by priorities outside the bedroom, such as building a marriage, raising a family, and launching a career. However, midlife may prove to be a turning point. Upon reaching menopause, the long-unsatisfied woman might greet the physical changes in her body as a sign that her sexual duties are fulfilled. If her husband is still interested in sex, a conflict is likely to erupt.
A much more hopeful scenario is also possible. Midlife and later may be a time when a woman’s sexuality blossoms. Menopause means that women no longer have to worry about pregnancy. Often, children are grown and family responsibilities have eased, allowing a couple to engage in more relaxed and spontaneous lovemaking. In addition, the changes a man is experiencing during these years, such as slower erections and longer time before ejaculation, lend themselves to the kind of pleasurable play that a woman may have been missing out on before.
For a couple wishing to embark on the more positive course, the key is to begin to unravel negative patterns. To do this, you must open up a dialogue. It’s also important to resist succumbing to unproductive beliefs about aging and sex.
Stress and lifestyle issues
Stress and fatigue are major libido sappers. During midlife, stress can hit from any direction and take any form. Challenging teenagers, financial worries, aging parents, and career woes are common. Concern over your own health or that of a loved one, or general anxiety about aging can also weigh heavily. With so many demands on your time and attention, you and your partner may neglect to nurture your relationship. This inattention can cause your sexual connection to fray as well.
Sheer lack of time is often a major factor. The physical changes in sexual response that occur in both men and women as they age mean that it will take you and your partner more time to become aroused and reach orgasm than it did in your younger years. You may find it hard to squeeze an extended lovemaking session into an already packed day. If a couple typically waits until bedtime to have sex, exhaustion also can become an obstacle.
Stress has a particularly deleterious effect on libido, especially in women. Whereas men can sometimes use sex to relax, women more often need to be relaxed in order to enjoy sex. This mismatch can create conflict for a couple.
Sexual issues brought on solely by stress and fatigue often can be remedied simply by taking a vacation. If you and your partner are able to resume pleasurable lovemaking in a pressure-free environment, you’ll be reassured that the underpinnings of your sexual relationship are sound.
Midlife and after is also a time when profound lifestyle changes take place. Events such as retirement and children leaving home can upset decades-long patterns in a couple’s life. For example, many couples go through a period of adjustment when they retire. If a woman is used to having the house to herself, her feeling of control over her domain can be threatened by her husband’s constant presence. If both partners worked outside the home, they must each adapt to having more time together at home.
One bonus is that retirement may allow you and your partner the opportunity to engage in leisurely lovemaking — something you may have lacked for many years. One danger, however, is that couples who begin spending a lot of time together may stop making an effort to include romance in their relationship.
Chronic illness also affects many couples’ sexual relationships during this stage of life. People who are ill may find that a condition or its treatment causes sexual difficulties, while healthy partners may worry that sexual activity will make their loved one’s condition worse. The fatigue and stress of the caretaker role may also dampen desire. In addition, sexual interest may wane for both partners if their caretaker−patient relationship begins to feel too much like that of a parent and child. During this time, many people also experience the loss of someone close — parents, friends, or siblings. Grieving may make it difficult to enjoy anything pleasurable, including sex.
Sexuality and Men: Lifestyle, health related to a good sex life as men age
For 20 years, the Harvard Health Professionals Follow-up Study has gathered important information about men’s health. In 2000, it added questions about sexuality to its semiannual surveys. According to the Harvard Men’s Health Watch, the new data offer insight on how men can maintain a satisfying sex life as they age.
Chronic illness and the medications used to treat them account for many of the sexual problems of older men. Sexual dysfunction was most prevalent in men with illnesses such as diabetes, hypertension, heart disease, stroke, and even depression. The Harvard Men’s Health Watch points out that one of the striking results of the study was that men with prostate cancer are 10–15 times more likely to experience sexual dysfunction than men without the disease—however, these sexual difficulties typically stem from the treatment rather than the cancer itself.
Even in healthy men, each aspect of sexual function showed progressive problems with age. Although libido decreased with age, sexual desire was preserved substantially better than erectile function. Although testosterone levels fall just as many men begin to experience sexual dysfunction, the Harvard Men’s Health Watch reports that most men have plenty of testosterone to spare—levels remain in the normal range in at least 75% of senior citizens.
“All in all, men who remain well are less likely to develop sexual dysfunction with age than men who fall ill,” says Harvey B. Simon, M.D., editor of the Harvard Men’s Health Watch. “And men who take good care of themselves enjoy substantial protection from both illness and sexual decline. The secret to preserving sexuality is to stay healthy and to build healthy relationships—and both require a series of wise choices throughout life.”
Sexuality and seniority
Americans are living longer than ever. As the population ages, many senior citizens are burdened with chronic illnesses, but many others remain healthy and active. When scientists investigate aging, they have to distinguish between changes caused by disease and those caused by aging itself. It’s important research: among other things, it has taught us that men who take care of themselves can prevent many of the illnesses that make less prudent gents old before their time.
Until recently, research on aging has focused mainly on crucial things that go wrong — on heart disease, mental decline, arthritis, prostate woes, and the like. But while big-ticket items are still getting the priority they deserve, researchers are also expanding their horizons to include less critical issues. Sexuality is an important example. Several reports shed light on aging and sexuality, and one of them suggests that sex itself may help prevent sexual dysfunction in older men.
The male sexual response
At any age, sexual activity is an instinctive, automatic part of human behavior. But the biology behind that behavior is quite complex.
Although the sex act is a continuous process, researchers have divided it into six stages. The first necessity is sexual desire or libido. The normal sex drive is a prime example of the unity of mind and body. It requires both an appropriate mindset and sufficient amounts of the male hormone testosterone. Sexual desires surface in puberty, when testosterone levels rise; although ardor tends to wane with age, most men produce enough testosterone to maintain libido throughout life. At any stage of life, however, worry, stress, or depression can thwart sexual interest, even if a man’s physical apparatus remains intact.
Sexual activity itself begins with a state of arousal that results from various combinations of erotic thoughts and sensory stimulation that may involve the senses of touch, sight, scent, taste, or hearing. An area of the brain called the hypothalamus co-ordinates erotic images and sensations and transmits the impulses of desire through the spinal cord to the pelvis, where they link up with the nerves of the autonomic nervous system; sensory nerves from the skin of the penis and other erogenous zones connect directly to the autonomic nerves without involving the brain.
When properly stimulated, the autonomic nerves in the pelvis spring into action. They start the second stage of the male sexual response by transmitting chemical signals to the arteries of the penis, causing them to widen and admit more blood. Blood rushes into the two corpora cavernosa, shafts of spongy tissue that contain many vascular channels. The corpora cavernosa swell, producing an erection. The engorged corpora also put pressure on venules, compressing and narrowing them to prevent the extra blood from leaving, so the erection can be maintained.
For years, doctors have known that an erection is a hydraulic event that depends on a sixfold increase in the amount of blood in the penis. But research has revealed that an erection is also a chemical event. A tiny chemical called nitric oxide allows nerves to communicate with each other and with the arteries of the penis. Nitric oxide acts on the arteries through an intermediary called cyclic guanosine monophosphate (cGMP). It’s been an exciting discovery for scientists, and it led to important progress for men with erectile dysfunction (ED) since the ED pills (Cialis, Levitra, and Viagra) act by boosting cGMP levels in the penis.
The third stage of sexual activity is called the plateau, which usually lasts from 30 seconds to two minutes. The heart rate and blood pressure rise as sexual activities continue, pumping more blood to the body’s tissues. The penis is not the only recipient of increased blood flow; most men also experience facial flushing, and the testicles themselves swell by about 50%. During the plateau phase, the prostate and seminal vesicles begin to discharge fluid in preparation for ejaculation.
Sexual excitement climaxes with the fourth stage, ejaculation. The autonomic nervous system is in charge here, too. It tells the muscles in the epididymis, vas deferens, seminal vesicles, and prostate to contract, propelling semen forward. At the same time, nerve impulses tighten muscles in the neck of the bladder so that semen is forced out through the urethra instead of flowing back into the bladder. Ejaculation is usually accompanied by the pleasurable sensation of orgasm; in nearly all men, the heart rate reaches its peak during ejaculation.
All good things come to an end. The fifth stage of sexual activity is detumescence, when the penis returns to its flaccid state. Detumescence usually follows ejaculation, but it can occur prematurely if the sex act is interrupted by an intrusive thought or event. In either case, detumescence occurs when the penile arteries narrow and the veins widen, draining blood away from the organ.
The final stage in the sex act is the quietest. It’s the refractory period, a span of 30 minutes (in younger men) to three hours (in older men) during which the penis cannot respond to sexual stimulation.
Slowing down
For many men, sexuality is one of the things that change over time. It’s usually a gradual, almost imperceptible process that begins in middle age. Whereas most older men retain an interest in sex, it’s generally a far cry from the preoccupation with sex that’s so common in youth. Although interest is retained, desire tends to wane; many older men think about sex, but don’t have the drive to put theory into practice. And even when the spirit is willing, the flesh may be weak; male sexual performance typically declines more rapidly than either interest or desire.
Most men experience decreased sexual responsiveness with increasing age. Erections occur more slowly, and they become more dependent on physical stimulation than on erotic thoughts. Even when erections develop, most men in their 60s report that their penile rigidity is diminished and harder to sustain. The ejaculatory phase also changes with age; the muscular contractions of orgasm are less intense, ejaculation is slower and less urgent, and semen volume declines. Sperm counts also decline; although healthy men can father children well into their senior years, their reproductive efficiency can’t match younger men’s.
Sexual intercourse requires a partner. But male sexuality demonstrates age-related changes that are not dependent on interpersonal factors. Nighttime erections, which are normal events that occur during deep sleep, diminish with age; men between age 45 and 54 average 3.3 erections per night; between age 65 and 75, men average 2.3. Nocturnal erections also tend to become briefer and less rigid as men age.
Changes due to age
Sexuality is complex, and scientists don’t understand all the factors that contribute to sexual function in young men, let alone what is responsible for the changes that occur with healthy aging. Still, it’s clear that the hormones, nerves, and blood vessels responsible for male sexuality all change over time. In the average man, levels of testosterone fall by about 1% per year beyond age 40 — but most older men still have enough testosterone to function sexually. To produce arousal, testosterone acts on part of the brain called the locus ceruleus, and these nerve cells become less hormone-responsive with age. Levels of estradiol, a predominantly female hormone, tend to decline with age; levels of another female hormone, prolactin, tend to rise. As for nerve function, penile responsiveness to sensory stimulation also slows with age. In addition, penile blood flow may decrease as men grow older, even if they stay healthy.
Changes due to illness
In men who stay well, all these changes add up to a gradual, partial decline in sexual activity. But in some men, the shift is more abrupt and complete. ED is closely linked to age. Only 5% of men under 40 years of age experience ED, but the prevalence rises steadily with age. About 44% of men in their 60s have ED, and the problem may affect up to 70% of American men over 70.
Because ED is so common in older men, many assume that it’s part of the normal aging process. It’s not. Instead, ED reflects the impact of chronic diseases that become increasingly prevalent with age. The most important are atherosclerosis and hypertension, which affect blood vessels, and diabetes, which strikes both blood vessels and nerves. In addition, stress, depression, and anxiety about adequate sexual performance can reduce sexual activity and satisfaction at any age. So too can marital strife, poor communication, poor sexual technique, and boredom; many of these problems become more common with age. Still, both partners in a relationship can expect to experience intimacy and sexual activity in maturity; if these expectations are not met, both people should explore the problems that may be responsible and the remedies that may be available. Important, too, are the medications that many older men require; numerous drugs can interfere with sexual function, including many used to treat high blood pressure, heart disease, anxiety, and depression.
Sexual surveys
Although you’d never guess it from late-night talk shows, TV ads for ED pills, or Mae West (“A hard man is good to find”), erectile dysfunction is not the only measure of successful male sexuality. Two surveys of sexuality in older men paint a more nuanced picture.
An American survey evaluated 1,455 men 57 to 85 years of age. Nearly 84% of men under 65 reported sexual activity with a partner during the year prior to the survey, but the figure fell to 67% in men between 65 and 74 and to 39% between 75 and 85 years of age. But among sexually active men, most reported at least two to three encounters per month throughout the three age ranges. There was little decline in sexual interest between ages 57 and 85, with over 70% of men maintaining interest. Confirming Shakespeare’s insight (“Is it not strange that desire should so many years outlive performance?”), however, ED became more common over the years. In all, 14% of the men reported taking medication or supplements for sexual dysfunction.
A Swedish survey evaluated 225 70-year-old men. Among the men who were living with a partner, 66% reported sexual intercourse within the previous year; of these, 31% reported intercourse one or more times per week. More than half of all the 70-year- old men reported that sexuality contributed to happy relationships.
Troubleshooting
In the age of Viagra, many men, young and old, respond to sexual dysfunction by downing a little blue pill or one of Viagra’s newer rivals. Indeed, the ED pills have been a tremendous boon to male sexuality, psychological health, and relationships. But men with sexual dysfunction should always work with their doctors to identify underlying causes of the problem — and when the issue is ED, it’s particularly important to identify and treat or correct cardiovascular risk factors, including abnormal cholesterol levels, high blood pressure, diabetes, tobacco abuse, obesity, and lack of exercise. In fact, ED is a powerful predictor of future heart disease, even in men who have no cardiac symptoms.
Keeping it up
Although treatment can help remedy sexual dysfunction, prevention is surely the best medicine. A 2003 Harvard study of 31,742 men between 53 and 90 emphasizes the preventive power of avoiding tobacco, getting regular exercise, staying lean, and avoiding excessive alcohol. And without contradicting these key instructions, a study suggests that sexual activity itself may help preserve erectile function in older men.
Sex “therapy”?
To find out if sexual intercourse protects against developing ED, scientists in Finland evaluated 989 men between 55 and 75. None of the men had ED when they volunteered for the study, and over 80% were married or living with a partner. Over the next five years, men who reported having intercourse less than once a week at the start of the study were more than twice as likely to develop ED as men who had intercourse weekly; they were also over four times more likely to develop ED than the men who reported having intercourse three times a week at the start of the study.
The study shows that men who are sexually active are less likely to develop ED than men who are less sexually active. But which is the horse and which the cart? Did increased sexual activity actually protect men from ED, or were men with good erectile function simply more active because they had better sexual function to begin with? The Finnish researchers tried to answer the question by evaluating the volunteers for problems that are linked to ED, including smoking, obesity, heart disease, high blood pressure, diabetes, depression, and cerebrovascular disease. Because they found little difference in ED risk factors among the groups, they argue that the crucial difference that protected against ED was sexual activity itself. Unfortunately, the study did not evaluate the possible impact of exercise, which lowers the risk of ED, or alcohol abuse, which raises risk.
The scientists offered a biological explanation for the apparent protective effect of sexual activity: erections bring oxygen-rich blood to the penis, perhaps preserving the health of tissues. It’s the theory behind the still unproven practice of using ED pills for “penile rehabilitation” in men with ED following prostate surgery. It’s an interesting theory, but more research is needed to see if it’s right. Since healthy men have two to three erections each night, it’s not clear that one to three acts of sexual intercourse per week would provide important extra benefit. The Finnish study did not evaluate nighttime erections, but it did report that the sexually active and less sexually active men had similar numbers of early morning erections.
Sex and age
Sexuality is an important aspect of life, but its role changes over time. Sex is necessary for procreation, which preserves the life of the species. And a healthy lifestyle is the best way to preserve sexuality in seniority. Most men remain interested in sex as they age, but many experience a diminished urge for sex and altered sexual function. Despite these changes, healthy men should expect to retain the capacity for sexual activity and satisfaction throughout life. The Finnish study suggests that regular sexual activity may help preserve erectile function as men age. Many men will welcome that finding, but more research is needed. At present, the best way to preserve sexuality is to preserve health; a good diet, regular exercise, and good health habits are the most effective ways to reduce the risk of developing the chronic diseases and requiring the medications that so often impair sexuality
Life after 50: A Harvard study of male sexuality
Even the most optimistic men know that the clock ticks for all of us. With each passing year, our bodies change, as does our behavior.
It’s certainly no surprise that male sexuality changes over time. Some 400 years ago Shakespeare asked, “Is it not strange that desire should so many years outlive performance?” Still, a major Harvard study of male sexual function in maturity does contain some surprises. It reports that sexual dysfunction is common and increases rapidly as men age. But it also says that simple lifestyle choices can slow the tick of the clock for many of us.
The Harvard study
Until Viagra burst onto the scene in 1998, few men were willing to discuss sexual problems. But the little blue pill and Senator Bob Dole changed all that, and researchers took advantage of the new openness to conduct a study of age and male sexuality.
The subjects were 31,742 men between the ages of 53 and 90. As members of the Health Professionals Follow-up Study, all were dentists, optometrists, osteopaths, podiatrists, pharmacists, or veterinarians. That makes them knowledgeable observers and reliable reporters of their health, but they do not reflect the broader U.S. population in terms of education, income, and race.
Since it began in 1986, the study has been gathering an enormous amount of information, and in 2000, it added sexuality to its semiannual surveys. Each man answered questions about his sexual desire, his ability to sustain an erection satisfactorily for intercourse, his ability to reach orgasm, and his overall sexual function. Because the database also contains details about each man’s general health, medications, and health habits, the scientists were able to evaluate sexuality in terms of health and lifestyle as well as age.
The toll of time
One of the striking results of the study was that men with prostate cancer are 10–15 times more likely to experience sexual dysfunction than men without the disease. In nearly all cases, the sexual difficulties stem from the treatment rather than the cancer itself. But since the incidence of prostate cancer increases steadily with age, it could skew the results of the analysis. To avoid confusion, the study excluded men with prostate cancer from the final tabulation, though it did include all other medical conditions.
Even in men without prostate cancer, the prevalence of sexual problems was very high: 29% reported moderate or severe difficulties. But not all age groups were equally affected; major problems rose from 10% in men younger than 59 years to 23% in 60- to 69-year-olds, 47% in 70- to 79-year-olds, and 64% in men 80 and over.
Each aspect of sexual function showed progressive problems with age. Fully a third of the men reported moderate to severe erectile dysfunction; but only 2% remembered that their difficulty began before the age of 40 and only 4% reported that it developed between 40 and 49. After 50, the number of men with the problem rose steeply from 26% between 50 and 59 all the way to 61% after 70. And as usual, Shakespeare got it right; although libido also decreased with age, sexual desire was preserved substantially better than erectile function.
| Testosterone and male sexuality
The male hormone testosterone is necessary for the development of male genital structures during fetal life. It triggers the dramatic events of puberty, and it is necessary for libido, sexual function, and fertility throughout maturity. Testosterone levels peak at about age 17, then remain high for the next few decades. But after the age of 40, testosterone levels fall by about 1% a year. That doesn’t sound like much, but by the age of 70 or so, it adds up to a 30% decline. Testosterone levels fall just as many men begin to experience sexual dysfunction. But that doesn’t make testosterone responsible for the problem. In fact, most men have plenty of testosterone to spare, so levels remain in the normal range in at least 75% of senior citizens. Testosterone patches and gels are increasingly popular among older men; doctors write more than a million such prescriptions a year, and the number is increasing rapidly. In addition, many men take weaker male hormones such as dehydroepiandrosterone (DHEA) and androstenedione (Andro) that are sold with-out a prescription as “dietary supplements.” It’s not a good idea. There is no evidence that male hormones will improve sexual performance in healthy men, and by stimulating the prostate, they may do more harm than good. Men who are truly testosterone deficient (hypogonadism) have diminished sexual interest and desire as well as erectile dysfunction. They can benefit from testosterone replacement therapy, but only after careful medical tests establish a diagnosis of testicular insufficiency. |
The toll of illness
Sexuality is not the only thing that changes with age. Chronic illnesses also become more common, and in each age group, sexual dysfunction was most prevalent in men with illnesses such as diabetes, hypertension, heart disease, cancer (other than prostate cancer), and stroke.
All in all, men who remain well are less likely to develop sexual dysfunction with age than men who fall ill. And men who take good care of themselves enjoy substantial protection from both illness and sexual decline.
The benefits of healthful choices
No man chooses to get sick, but many choose behaviors that boost their odds of becoming ill. Although the health professionals who participated in the study should have known better, some didn’t — and they paid the price in terms of impaired sexual function as well as illness. The risk of sexual problems was linked to smoking, obesity, heavy drinking, and the time spent watching television. In contrast, regular physical exercise and moderate alcohol consumption help preserve good sexual function. In this respect, the study agrees with earlier research showing that erectile dysfunction can be prevented.
Age and sexuality
The Harvard study of male sexuality and age is the largest of its kind and provides important confirmation of earlier research as well as additional interesting information. Chronic illness and the medications used to treat them account for many of the sexual problems of older men; depression can also take a toll. But even in healthy men, a slow change in sexuality begins in middle age and continues throughout life. Whereas most older men retain an interest in sex, it is generally a far cry from the preoccupation with sex that is so common in youth. Although interest is retained, desire tends to wane; many older men think about sex but do not have the drive to put theory into practice. And even when the spirit is willing, the flesh may be weak; male sexual performance typically declines more rapidly than either interest or desire. Most men experience decreased sexual responsiveness with increasing age. Erections occur more slowly, and they depend more on physical stimulation than erotic thoughts. Even when erections develop, most men in their sixties report that their penile rigidity is diminished and harder to sustain. The ejaculatory phase also changes with age. The muscular contractions of orgasm are less intense, ejaculation is slower and less urgent, and there is a longer refractory period following intercourse, when men cannot respond to sexual stimulation. Semen volume and sperm counts decline, as does fertility.
The study evaluated sexuality but not relationships. Sexual intercourse requires a partner, but male sexuality demonstrates age-related changes that do not depend on interpersonal factors. Nocturnal erections diminish with age; men between 45 and 54 average 3.3 erections per night; between 65 and 75, they average 2.3 erections. Nocturnal erections also tend to become briefer and less rigid with age.
Life may not begin at 80, but sex life doesn’t automatically end with advancing age. Many surveys report that the frequency of sexual activity declines, but they disagree about how often older couples have intercourse. In round numbers, 50%–80% of healthy couples over 70 report sexual activity on a regular basis, including weekly intercourse in about half of them.
The secret to preserving sexuality is to stay healthy and to build healthy relationships — and both require a series of wise choices throughout life.
Sex in the second half
Sex isn’t just for the young. Research is showing that older Americans are sexually active.
The sexuality that’s such a big part of our teens and young adulthood has more staying power than younger people usually recognize and can continue to spice things up well into old age. Results from a University of Chicago survey published in 2007 suggested that over half of Americans continue to engage in sexual activities well into their 70s. Now another batch of findings from a survey conducted by researchers at Indiana University suggests that 20% to 30% of long-lived Americans are sexually active into their 80s.
Both of these surveys are cross-sectional — snapshots of behavior in a given period — so making pronouncements about trends would be getting ahead of the evidence. Still, there’s reason to believe that sexuality is assuming a larger role in American old age. Millions of men are now taking erectile dysfunction drugs like sildenafil (Viagra) or tadalafil (Cialis). Growing numbers of Americans are enjoying relatively good health in their 60s, 70s, and 80s, and, not surprisingly, the University of Chicago study found a close association between good health and sexual activity among older people.
Consider also who is getting old these days — the baby boomers, a generation that came of age in the 1960s and ’70s when sexual mores were changing, and a demographic group that hangs on to its youthful ways.
But the “frisky seniors” story line can be overdone. Sexual activity does subside with age. Biological factors tug in that direction, as do social arrangements: older people, especially women, often end up single when a spouse or partner dies. The Indiana University researchers found that sexual activity with a partner is common among those in their 20s, 30s, and 40s, dips significantly for both men and women in their 50s and 60s, and then drops further once people enter their 70s.
Now suitable for study
It wasn’t long ago that older people weren’t included in studies of sexual behavior because they were seen as largely irrelevant to the topic: 59 was the upper age limit of a landmark study of American sexuality conducted in the early 1990s. The University of Chicago survey (the formal name is the National Social Life, Health, and Aging Project) went a long way toward rectifying the situation. It focused exclusively on older adults, including just over 3,000 Americans ages 57 to 85. The results, published in The New England Journal of Medicine in 2007, received a fair amount of attention and lent some legitimacy to the subject of sexuality of older people.
The Indiana University survey was conducted by the university’s Center for Sexual Health Promotion, which grew out of the research efforts of Dr. Alfred Kinsey in the 1940s and 1950s. Kinsey, who died in 1956, is credited with being one of the pioneers of research into human sexuality, although revelations about his research methods and personal life have since tarnished his reputation.
Kinsey and his colleagues conducted their research with in-depth interviews; this generation of Indiana sex researchers used electronic questionnaires and the Internet. A total of 5,865 Americans, ranging in age from 14 to 94, were included in the survey. A parent or legal guardian had to give permission for a teen to participate. Computers and Internet access were provided to the participants who didn’t have them.
Sophisticated sampling techniques are used in this kind of survey research to make sure the study volunteers accurately reflect the population’s age, income, geographic distribution, and other attributes. But sex researchers can’t overcome the problem of self-selection: the sort of people who agree to fill out such a questionnaire may not reflect the population as a whole, particularly when it comes to sexual behavior. There’s also no way of telling whether respondents are telling the truth about their behaviors, although the Indiana researchers point out that the anonymity of their Internet-based research may tend to make people more, not less, truthful about taboo subjects. The University of Chicago survey depended on in-home interviews.
Church & Dwight Co., the company that makes Trojan condoms, funded the Indiana University survey, and condom use featured prominently in the initial batch of survey-based articles published in a supplement to The Journal of Sexual Medicine in October 2010. One of them focused on the 1,973 respondents ages 50 and older, a third of the total.
A statistical picture of the sexuality of older Americans begins to emerge from that article and the University of Chicago survey results. Here are some of the main points:
Sexual activity tapers off with age. Both surveys show a decline in sexual activity with age, although the drop-off isn’t as steep as one might expect, and a significant minority (especially men) defies the trend. In the Indiana study, 35% of the men age 80 and older reported that they had intercourse with a woman a few times or more in the past year. In the University of Chicago study, 38.5% of the men ages 75 to 85 reported having sexual activity with a partner in the previous year.
Older women are less sexually active than older men. Both studies show that older women — even the “young old,” in their 60s — are less sexually active than men of the same age. The gender gap widens as people get older. The University of Chicago researchers noted that the women in their study were less likely than the men to be in a marital or intimate relationship, and even more so with age, presumably because men tend to die at a younger age than women. Differences in the amount of sexual activity that occurs outside of a relationship contribute to the overall gender disparity. In the University of Chicago study, about one in 20 women who were not in a relationship reported being sexually active in the previous year, compared with about one in five men who were not in a relationship.
Partnered sex gets high marks. In the Indiana study, over three-quarters (78%) of the men ages 50 and over rated their most recent sexual experience with a partner as either extremely or “quite a bit” pleasurable. About two-thirds (68.2%) of the women in that age group rated their most recent experience with a partner that highly.
Masturbation is common. Most men (63%) and almost half of women (47%) in the 50 and over age group reported masturbating in the past year, according to the Indiana survey. As with other sexual activities, the percentage declined with age, although a significant number of those 80 and older indicated that they masturbated.
The University of Chicago survey found masturbation to be almost equally common among those in a relationship and those not in one.
Good health matters. The University of Chicago researchers found a strong association between good health and sexual activity, particularly among men. Diabetes seems to have a greater negative effect than either arthritis or high blood pressure on both genders, but especially on women. In the Indiana survey, a woman’s evaluation of her last sexual experience did not vary with her self-reported health status.
Sexual problems are common. Half of those who participated in the University of Chicago study reported having at least one bothersome sexual problem. Among men, the problems included difficulty achieving and maintaining an erection (37%), lack of interest in sex (28%), anxiety about performance (27%), and inability to climax (20%). Among women, the common problems were lack of interest in sex (43%), difficulty with lubrication (39%), inability to climax (34%), lack of pleasure from sex (23%), and pain during sex (17%). In the Indiana survey, 30% of the women ages 50 and over said they experienced some level of pain during their most recent sexual experience with a partner.
The University of Chicago researchers also asked people whether they were bothered by their sexual problems. Men tended to be bothered by them more than women, although when it came to lack of interest in sex, the percentages were about the same: of those who had this problem, 65% of the men said they were bothered by it, compared with 61% of the women.
Sexual activity outside of a relationship is common. A sizable minority of the men (43%) and women (36%) in the Indiana study reported that their most recent partnered sexual activity was with someone other than a spouse or long-time partner. This “nonrelationship” partner category included casual or new acquaintances, friends, and “transactional” partners — people who engaged in sex in exchange for something, often but not always money. Women whose last sexual partner was with a nonrelationship partner reported higher arousal, less lubrication difficulty, and a higher rate of orgasm than women whose last partnered sexual activity was with a spouse or a long-time partner.
Many men take something to improve sexual function. In the Indiana survey, 17% of men ages 50 and older took an erectile dysfunction drug in connection with their most recent sexual experience with a partner. In the University of Chicago study, 14% of the men and 1% of the women reported taking medications or supplements to improve sexual function during the past year.
Age cuts both ways
So it’s pretty clear: old age doesn’t preclude sexual activity, although it also doesn’t make it any easier. Men experience declines in testosterone, which adversely affects sexual arousal and desire. There are age-related changes to blood vessels and smooth-muscle tissues that can make achieving an erection more difficult. Chronic conditions such as diabetes and high blood pressure become more common in old age, and in many men, they adversely affect erections more than any of the strictly age-related changes. Women are also affected by chronic illnesses, in addition to changes related to menopause, which include reduced vaginal lubrication associated with lower estrogen levels.
But age and experience may also hold some advantages. For example, some research suggests that women become more comfortable asserting themselves sexually as they get older. Some men gain greater control over ejaculation. It’s also easier now to overcome some of the physiological hurdles that occur with age. Men have the erectile dysfunction drugs. Women can use any number of vaginal creams and gels. In fact, the number of older people who are sexually active has doctors and public health officials concerned about unprotected sex and sexually transmitted diseases in the elderly. With sex comes responsibility, even if you’re old enough to collect Social Security.
The bladder workout
The bladder workout: Tame incontinence without surgery
 |
An overactive bladder (also known as urge incontinence) causes a sudden urge to urinate, even when your bladder isn’t full. For some people, it’s simply a nuisance. For others, the urge can’t be controlled, which leads not only to incontinence but also to a potentially severe negative impact on their quality of life.
Bladder training can go a long way toward helping with urinary incontinence. This treatment strategy involves learning to urinate on a schedule (timed voiding) and doing pelvic muscle exercises.
Here’s a step-by-step bladder-training technique:
- Keep a diary. For a day or two, keep track of the times you urinate or leak urine during the day.
- Calculate. On average, how many hours do you wait between visits to the bathroom during the day?
- Choose an interval. Based on your typical interval between needing to urinate, set your starting interval for training so that it’s 15 minutes longer. So, if you usually make it for one hour before you need to use the bathroom, make your starting interval one hour and 15 minutes.
- Hold back. On the day you start your training, empty your bladder first thing in the morning and don’t go again until you reach your target time interval. If the time arrives before you feel the urge, go anyway. If the urge hits first, remind yourself that your bladder isn’t really full, and use whatever techniques you can to delay going. Try pelvic floor exercises (also called Kegels), or simply try to wait another five minutes before walking slowly to the bathroom.
- Increase your interval. Once you are successful with your initial interval, increase it by another 15 minutes. Over several weeks or months, you may find you are able to wait much longer and that you feel the urge less often. After four to eight weeks, if you think you have improved, do another diary. Compare your initial diary to your second diary to note the improvements in your intervals and the amount of urine you void. The act of reviewing and comparing actually helps reinforce the bladder training process.
Neuro-biology of psychiatric brain disorder
It does not adequately inform psychiatric practitioners about the many clinical and biologic features shared across the various diagnostic categories. It does not do justice to the galloping advances in the neurobiology of psychiatric brain disorders and the wealth of potential biomarkers that will eventually endow psychiatry with an objective and ultimately more valid, not just reliable, diagnostic model that is compatible with a future of precision medicine.
The Research Domain Criteria (RDoC) Project1 is a valiant attempt to transcend the DSM’s “Chinese menu” approach to diagnosis. It was championed by the former director of the National Institute of Mental Health (NIMH), who used his authority to encourage investigators applying for federal grants to employ the RDoC principles in their research programs. Who does not recall the awkward moment, a few weeks before the official baptism of DSM-5 as psychiatry’s latest diagnostic Bible in May 2013? The NIMH director’s unflattering portrayal of the incipient DSM-5 was a well-publicized shot across the bow. The kerfuffle was later resolved, but its effects linger among clinical researchers who relentlessly hope for neuroscience advances to translate into a more objective diagnostic approach to psychiatric diagnoses. The neurobiological foundations of psychopathology are bound to guide us to a more valid set of diagnostic categories, yet the pace remains painfully slow.
However, the copious advances in brain research are providing other dividends beyond a better diagnostic forest. Many intriguing insights are emerging about the connectedness among major psychiatric “trees,” including schizophrenia, bipolar disorders, and major depressive disorder. The following are examples of neurobiology, clinical, and treatment commonalities across those psychotic and mood disorders.
Shared neurobiology
Progressive brain tissue loss/neurodegeneration.
Numerous studies have established that abnormal neuroplasticity is a common theme during psychotic, manic, and depressive episodes. These findings have demonstrated that the more recurrent the episodes, the more prominent the atrophy in either overall brain volume or specific brain regions, especially in the hippocampus, prefrontal cortex, and cerebellum as measured on MRI.
White matter pathology.
Multiple studies have reported a loss of myelin integrity in psychotic and mood disorders. Abnormalities are detected by using diffusion tensor imaging and measuring anisotropy and diffusivity of water flow in white matter traits. White matter pathology can be associated with intra- and inter-hemispheric disconnectivity and impairment of brain functional integration that may contribute to positive, negative, and cognitive symptoms.
Neuroinflammation.
Acute psychotic and mood episodes have been shown to be associated with significant elevation in inflammatory cytokines in CSF and serum, including interleukins (such as interleukin-6), tumor necrosis factor-alpha, interferon gamma, and C-reactive protein. Those inflammatory biomarkers subside when the acute episodes are treated. It is believed that activation of the microglia leads to a release of proinflammatory cytokines.
Mitochondrial dysfunction.
Many studies document various dysfunctions of the mitochondria in schizophrenia, bipolar disorders, and major depressive disorder. The consequences include oxidative stress due to a decrease in the antioxidant glutathione, produced in the mitochondria, which is vital for neutralizing the reactive oxygen and nitrogen species referred to as free radicals. There is a substantial increase of free radicals during acute psychotic and mood episodes, which contributes to neurodegeneration.
Glutamate pathway abnormalities.
A large body of literature has focused on the glutamate N-methyl-D-aspartate receptor (NMDAR) dysfunction as a key pathophysiology in schizophrenia and mood disorders. Interestingly, the NMDAR appears to be hypoactive in schizophrenia as evidenced by the schizophrenia-like effects of potent NMDAR antagonism by phencyclidine and hyperactive in unipolar and bipolar depression as evidenced by the remarkably rapid improvement of treatment-resistant depression with the NMDAR antagonists ketamine or nitrous oxide. Glutamate pathways may ultimately shed light on the neurochemical pathology underpinning psychotic and mood disorders. The NMDAR is also likely linked to both neuroplasticity and cognitive impairments in the major psychiatric disorders because both are related to calcium passing through the NMDAR ion channel
وصايا لقمان
Safeguard your feet
Stay ahead of foot problems by inspecting your feet regularly, keeping them flexible, and wearing the right shoes.
 Feet are the unsung heroes of mobility, and it’s crucial to keep them healthy. Even minor problems with your feet — such as an ingrown toenail or a small cut — can leave you sidelined. “Breaches of the skin can quickly become problems, whether it’s a scrape, ulcer, or blister that gets contaminated or becomes infected.
Feet are the unsung heroes of mobility, and it’s crucial to keep them healthy. Even minor problems with your feet — such as an ingrown toenail or a small cut — can leave you sidelined. “Breaches of the skin can quickly become problems, whether it’s a scrape, ulcer, or blister that gets contaminated or becomes infected.
Be proactive, and care for your feet the way you’d maintain any valuable equipment you rely on for mobility. Here are seven ideas to help.
1. Inspect your feet daily
Make foot exams part of your daily routine. Examine the tops and bottoms of your feet. Use a mirror if you can’t see the bottoms well. “Look for anything unusual: skin changes, cuts, blisters, drainage, an ulcer, a splinter, or what looks like a spot of dirt that on closer inspection could be a small tick. Watch for discoloration of the toenails, too, which can indicate problems such as a fungal infection.
2. Take care of toenails
It’s important to keep your toenails trimmed. Long toenails can scratch other toes or cause infection. If your toenails touch the end of your shoe, you can get a blood clot under the nail that can cause it to fall off or be very painful. As you get older and stiffer, it can become harder to reach and trim your toenails. Get regular pedicures from a podiatrist or a reputable salon, if you cannot perform this routine care yourself. How often depends on how fast your toenails grow.
3. Don’t go barefoot
Infections from untreated wounds on the bottoms of the feet are common. These are often from people walking barefoot. Wear shoes with socks to cut down on irritation. In public showers, wear flip-flops to prevent contracting plantar warts or fungal infections. Plantar warts are growths caused by the human papillomavirus, which gets into the skin of the feet through open areas or cuts.
4. Wear the right shoes
“People typically buy shoes that are fashionable but not functional. That makes foot problems worse,” says Dr. DiGiovanni. Look for shoes with a wide, roomy toe area; a sturdy heel counter (the area of the shoe around your heel); and a wide, flexible sole. The shoe should extend in length about half an inch beyond your longest toe. Dr. DiGiovanni recommends against using store-bought orthotics unless your doctor thinks it is a good idea.
5. Keep your feet flexible
The tissues in the feet get stiffer as we get older. That can lead to plantar fasciitis or heel pain. Plantar fasciitis is inflammation of the band of tissue that extends along the bottom of the foot.
One of the best ways to prevent such foot problems is by exercising regularly and doing daily foot strengthening exercises or stretches. “I tell my patients to go swimming, to cycle, or to do yoga. That helps keep the feet healthy and stretched out,” says Dr. DiGiovanni.
To keep feet supple, sit in a chair, lift one foot up, and try tracing each letter of the alphabet in the air with your toe. Repeat with the other foot. For a toe stretch, place the side of your foot on your knee and pull your toes upward,” suggests Dr. DiGiovanni.
After exercising, try calf stretches: Stand about 12 inches in front of a wall, and then lean toward the wall while keeping your heels on the ground. Hold the stretch for about 30 seconds.
6. Listen to your feet
If you’re exercising and develop sudden pain, redness, or swelling in your feet that doesn’t go away, rest them. If the problem doesn’t resolve within a few days to a week, seek advice from an expert.
Paroxetin : the story short
Pain relief techniques

Sometimes pain has a purpose — it can alert us that we’ve sprained an ankle, for example. But for many people, pain can linger for weeks or even months, causing needless suffering and interfering with the quality of life.
If your pain has overstayed its welcome, you should know that you have more treatment options today than ever before. Here, we’ve listed eight techniques to control and reduce your pain that doesn’t require an invasive procedure — or even taking a pill.
1. Cold and heat.
These two tried-and-true methods are still the cornerstone of relieving pain for certain kinds of injuries. If a homemade hot or cold pack doesn’t do the trick, try asking a physical therapist or chiropractor for their versions of these treatments, which can penetrate deeper into the muscle and tissue.
2. Exercise.

Physical activity plays a crucial role in interrupting the “vicious cycle” of pain and reduced mobility found in some chronic conditions such as arthritis and fibromyalgia. Try gentle aerobic activities such as walking, swimming, or cycling.
3. Physical therapy and occupational therapy.
These two specialties can be among your staunchest allies in the fight against pain. Physical therapists guide you through a series of exercises designed to preserve or improve your strength and mobility. Occupational therapists help you learn to perform a range of daily activities in a way that doesn’t aggravate your pain.
4. Mind-body techniques.

These techniques, which include meditation, mindfulness, and breathing exercises (among many others), help you restore a sense of control over your body and turn down the “fight or flight” response, which can worsen chronic muscle tension and pain.
5. Yoga and tai chi.

These two exercise practices incorporate breath control, meditation, and gentle movements to stretch and strengthen muscles. Many studies have shown that they can help people manage pain caused by a host of conditions, from headaches to arthritis to lingering injuries.
6. Biofeedback.

This technique involves learning relaxation and breathing exercises with the help of a biofeedback machine, which turns data on physiological functions (such as heart rate and blood pressure) into visual cues such as a graph, a blinking light, or even an animation. Watching and modifying the visualizations gives you a degree of control over your body’s response to pain.
7. Music therapy.
Studies have shown that music can help relieve pain during and after surgery and childbirth. Classical music has proven to work especially well, but there’s no harm in trying your favorite genre — listening to any kind of music can distract you from pain or discomfort.
8. Therapeutic Massage.

Not just an indulgence, massage can ease the pain by working tension out of muscles and joints, relieving stress and anxiety, and possibly helping to distract you from pain by introducing a “competing” sensation that overrides pain signals.
Antidepressants medication: they work but what to do with side effects?

Antidepressant medications can be a godsend for people struggling with the dark mantle of depression. Yet like all drugs, they can cause side effects, which is why it’s important to be aware of any changes in your body when you begin any new medication.
If you have any uncomfortable or worrisome antidepressant side effects, tell your doctor immediately. But for many of the mildly distressing side effects, a few simple steps may help. Here are some suggestions for managing side effects of antidepressants.
Dry mouth.

Drink a lot of water, chew sugarless gum, and brush your teeth frequently.
Constipation.

Eat whole grains, bran cereal, prunes, and hearty servings of fruits and vegetables. Drink plenty of water.
Trouble urinating.


If you have difficulty starting urination, your doctor may be able to adjust your medication to relieve this problem.
Dizziness.


Sudden changes in position can lead to a sharp drop in blood pressure that causes dizziness. To counter this effect, move slowly when you rise from a chair or get out of bed. Also, drink plenty of fluids.
Daytime drowsiness.


This problem usually occurs at the beginning of treatment and may not last long. In some cases, it may help to take medication at bedtime, but ask your doctor about this first. If you feel drowsy, don’t drive or use the heavy or dangerous equipment.
Trouble sleeping.


Sleep often improves after a few weeks, but sometimes a mild sleep aid or a switch to another medication is necessary.
Nausea.

Often, nausea disappears within a few weeks. It may help to take the drug shortly after a substantial meal.
Agitation.



You might feel uncomfortably nervous or restless after you start taking a drug. Jittery feelings may pass within a few weeks. But in relatively rare cases, agitation will persist; sometimes it’s an early symptom of worsening depression or mania.
Headache.


Headaches may come and go. Some persist, but they usually disappear within a few weeks.
Sexual difficulties.


Sometimes sexual problems are transient or not related to the drug. Talk with your doctor about sexual problems that persist for more than a few weeks.
Sometimes sexual problems are transient or not related to the drug. Talk with your doctor about sexual problems that persist for more than a few weeks.
If any antidepressant side effects continue to bother you, your doctor may change your dose, shift the time of day that you take the medication, or split the daily dose into smaller amounts to be taken over the course of the day. Or he or she may recommend combining the drug with another one, switching to a different drug, or replacing drugs with therapy or other forms of treatment. Take all medications as directed, and don’t stop taking them abruptly without talking to your doctor first.
كلمتنا في الادمان

يمزح الناس أحيانا في استخدام مصطلح “الإدمان” في المحادثات اليومية،
ويشير البعض إلى أنفسهم على أنهم “مدمن الشوكولاته” أو “الكورن فليكس ” أو السلمون ..وهكذا .
ولكنيجب أخذ الإدمان شيئا على محمل الجد.
الإدمان على الكحول، الماريجوانا، الأدوية وصفة طبية، القمار، الحبيبة أو الحبيب
وغيرها من المواد أو الأنشطة أو الشخصيات
يمكن أن يسبب مشاكل صحية خطيرة ومشاكل مع أفراد الأسرة والأصدقاء وزملاء العمل والعمل والمال والقانون.
ومع ذلك، وعلى الرغم من هذه المشاكل، لا يزال الشخص يستخدم المادة أو ينخرط في النشاط المؤذي أو العشق المستحيل
الناس الذين يعانون من إدمان تميل إلى إظهار ثلاثة شعور وسلوك وتفاعل :
فأما الشعور فهو ..حنين للكائن من الإدمان، والتي يمكن أن تكون خفيفة إلى مكثفة
يمكنك ان تسميه شغف أو لهفة أو اشتياق أو حتى و حم
و أما السلوك فهو
فقدان السيطرة على هذا الشغف أو اللهفة
فهو و أما التفاعل
استمرار التعامل مع موضوع الإدمان و التقلب في التقارب نه على الرغم من العواقب الضارةالمعروفة لذلك
الإدمان
في تعريفه الأساسي
هو الاعتماد المادي على مادة أو نشاط أو شخص يؤدي هذا الاعتماد إلى أعراض غير سارة ، تسمى أعراض الانسحاب أو الافتراق أو الابتعاد ، التي تظهر عندما يتوقف الشخص عن استخدام أو المادة أو القيام بالنشاط. أو الاقتراب من الحبيب
لا أحد يرغب في تطوير الإدمان.
ولكن بعض الناس ينجذبون لبعض المواد أو السلوكيات لأسباب محددة.
معظم هذه المدمنات أي الأشياء التي ندمنها تقدم للناس بعض المكافآت النفسية والاجتماعية مثلا راحه نفسية ..انسجام .. تضيع للوقت ..سرعة في الفكر ..ثقة بالنفس ..نوم مشبع..غزارة أفكار . سولة صحبة .. كياسة أخلاقية هذه المكافآت غالبا ما تكون مقنعة للمتعاطي أو المجرب في الأيام الأولى ، وبالتالي فهي جذابة له حتى لو كانت فيها تكلفة. باهظة
ومن العناصر الرئيسية للتغلب على الإدمان الاعتراف بالقيمة المضافة .للمدمن من جراء التعاطي .. ماذا تضيف هذه المادة الى
بمجرد فهم القيمة التي تستمدها من الإدمان الخاص بك،
يمكنك البحث عن بديل -يكون أقل تدميرا – و تأكد تمكن منك الداء فهناك الدواء.
.. و أفضل عادة ألا تكون مدمن عادة
فلا تكون أسير نفسك حتى مع من تعشق وأنت تعلم انه عشق و حب يائس عقيم
Brief word about Addiction
walking tips

Warm weather is here, and you may be walking more to take advantage of being outside. Why not ramp up your routine with bursts of fast-paced walking? The technique, known as interval walking, “is a great way to get the most exercise bang for your buck,” says Dr. Aaron Baggish, associate director of the Cardiovascular Performance Program at Harvard-affiliated Massachusetts General Hospital.
About interval training
Interval walking is a form of interval training, which describes any form of exercise in which you purposely speed up or slow down at regular intervals throughout the session. The benefits of interval training in athletes and people in cardiac rehabilitation are well studied. Dr. Baggish says interval walking hasn’t been examined as much, but he believes the same benefits apply. “Something about strenuous exercise is good for the body. It improves endurance, reduces blood pressure, and helps with weight loss,” he explains.
Interval training may also burn more calories, and help you get fit faster. For example, a small observational study published last year in PLOS ONE suggested that three 20-second sprints during a 10-minute cycling workout produced benefits similar to a 45-minute cycling workout.
Master the basics
Before attempting interval walking, first make sure that your doctor approves, especially if you have heart disease or joint pain. You’ll also need a solid walking program in place. “A well-established routine would be at least two or three months of being able to walk 20 to 30 minutes a day without any limitations,” says Dr. Baggish. Ideally, you should walk at least five days a week.
Also important: walk with a partner, for safety and motivation, and bring a cell phone in case you need to call for help.
Remember to dedicate five minutes each to warm-up and cool-down as part of the walking routine. This can simply involve walking at a comfortable pace.
Work your way up
When you’re ready to add interval walking to your routine, start slowly. Introduce one or two segments of fast-paced walking into your 30-minute walk. Each segment should last a minute or two. Try that during each walking workout for a few weeks.
How much should you pick up the pace during an interval? “Walk as fast as you can, at a pace you can do briefly, but can’t do forever,” suggests Dr. Baggish. He adds that you don’t have to worry about trying to reach a particular heart rate unless your doctor directs you to do so.
Gradually add more intervals into your routine, with an ultimate goal of walking 50% of the time at the higher intensity. There’s flexibility in how that can be done — one minute on, one minute off, or two minutes on, two minutes off. Play around with it, and see what’s best for your body.
The right path
The route you take will be particularly important when you’re interval walking since you won’t have as much time to avoid potential hazards if you’re pouring on the steam.
Look for smooth terrain in public areas. Neighborhoods, busy parks, and shopping malls are all good candidates for walking routes. Soft surfaces like dirt or grass are easier on the joints than asphalt or concrete.
You may also choose to do interval walking on a treadmill. Just crank up the speed or the incline for a minute or two to get your heart, lungs, and muscles working harder.
It also helps to know how far you’re walking. Find out by driving the route and using your car odometer, if the route is along neighborhood streets; using a pedometer; or calling the management office at a shopping mall, if you’re walking inside.
Final tips
Adding 60 seconds of fast-paced intervals to your routine will be tricky without a way to keep track of the time. That’s because it can be challenging to count silently when you hear the rhythm of your footsteps and breathing.
Save yourself the hassle; wear a watch with a second hand, or a digital watch with a stopwatch feature.
Harvard supplement
الكالسيوم و فيتامين د : ساحران العظام و توازن الحالة النفسية؟

تعد هشاشة العظام أو ضعف العظام أمر شائع جدا بين كبار السن، ولكنه ليس شيئا حتميا منه من الشيخوخة.هناك الكثير يمكنك القيام به لحماية العظام من هذا المرض.
أفضل تأمين ضد هشاشة العظام هو بناء أعلى كثافة ممكنة للعظام في عقد الثلاثينات من عمرك ثم تقليل فقدان العظام بعد ذلك.
ولكن إذا كنت بالفعل في منتصف العمر أو أبعد من ذلك، فما العمل
لا يزال هناك الكثير يمكنك القيام به للحفاظ على العظام لديك وربما حتى لاستبدال العظام المفقودة.

فممارسة الرياضية اليومية ورياضة رفع الاوزان على التحديد ، ويتضمن ذلك المشي الرياضي الصحي ..خطوة العسكرى مشدود الالكتاف و البطن و الالخطو على الكعب
، فهو أفضل دواء.
الحصول على ما يكفي من الكالسيوم وفيتامين د هما من الاستراتيجيات الهامة الأخرى للحفاظ على العظام قوية.
الكلسيوم

الكالسيوم هو عنصر غذائي مهم لبناء العظام وتباطؤ وتيرة فقدان العظام.
ولكنها ليست رصاصة سحرية واحدة، ويقترح بعض العلماء أن الكثير من الكالسيوم أو منتجات الألبان قد تكون غير صحية.
نضع في اعتبارنا أنه بالإضافة إلى الكالسيوم، هناك غيره من المواد الغذائية والأطعمة التي تساعد على الحفاظ على عظام قوية –
الأهم من فيتامين (د)، ولكن أيضا فيتامين K.
كم الكالسيوم؟

الكمية اليومية الموصى بها للكالسيوم هي 1000 ملليغرام (ملغ) يوميا للبالغين حتى سن 50 و 1200 ملغ يوميا للأشخاص الذين تتراوح أعمارهم بين 51 سنة وما فوق، عندما يسرع فقدان العظام. مع التقدم في العمر،
والأمعاء تمتص أقل الكالسيوم من النظام الغذائي، والكلى أقل كفاءة في الحفاظ على الكالسيوم. ونتيجة لذلك، يمكن لجسمك سرقة الكالسيوم من العظام لمجموعة متنوعة من وظائف التمثيل الغذائي الهامة.
من الناحية المثالية، يجب أن تحصل على الكالسيوم من خلال مصادر غذائية.
وتشير بعض الأبحاث إلى أن الحصول على الكثير من الكالسيوم من المكملات الغذائية قد يزيد من خطر الإصابة بأمراض القلب وسرطان البروستاتا.
ولذلك فمن الأفضل التحدث مع طبيبك إذا كنت تعتقد أنك بحاجة إلى الكالسيوم.

فيتامين د


في بناء العظام، والكالسيوم لديه مساعد لا غنى عنه: فيتامين (د) يساعد هذا الفيتامين الجسم على امتصاص الكالسيوم، ويعتقد بعض الباحثين أن زيادة فيتامين (د) يمكن أن تساعد في منع هشاشة العظام. الحليب المقوى في الولايات المتحدة محصن بفيتامين د. فيتامين (د) منتشر أيضا في حبوب الإفطار كالقمح (البليلة) والبيض والمكملات الفيتامينية. يتم تحصين بعض العلامات التجارية من الزبادي معها، وكذلك بعض العصائر.
وإذا أمكن، يمكن أن تساعد كمية صغيرة من التعرض لأشعة الشمس جسمك على تصنيع فيتامين D الخاص به – حوالي 5 إلى 30 دقيقة من ضوء الشمس بين الساعة 10 صباحا و 3 مساء. مرتين في الأسبوع على وجهك والذراعين والساقين، أو الظهر دون واقية من الشمس سوف تمكنك من جعل ما يكفي من فيتامين.
الناس الذين يعانون من الجلد الرقيق و الذي يحرق بسهولة تحت أشعة الشمس يكفي التعرض لأشعة الشمس إلى 10 دقيقة أو أقل.
يجب أن يكون الطعام والشمس كافيا، ولكن إن لم يكن، ينصح بعض الخبراء الحصول على 1،000 وحدة دولية من فيتامين D يوميا
نضيف الى ذلك توازن الحالة النفسية و فعالية العلاج الدوائي بشكل أفضل و الابتعاد عن شبح القلق و الاكتئاب ..يرتبط ارتباطا وثيقا بكفاءة فيتامين د المفعل بالجسم .. فالقلق و الاكتئاب مرتبط احصائيا بنقص فيتامين د بالجسم والكالسيوم عند الاطفال و المراهقين مرتبط بالتوازن الانفعالي و الحركي ونقصه يعطي مؤشرات شبيهه بحالات فرط الحركة و قصور الانتباه
كيف يمكن قياسها : كثافة أو هشاشة العظام

العديد من التقنيات يمكن تقييم كثافة العظام، ولكن الأكثر شيوعا المعروفة باسم الطاقة المزدوجة الأشعة السينية الممتصة (ديكسا) DEXA Dual Energy X-ray Absorptiometry .
في هذا الإجراء، يرسل جهاز الأشعة السينية أشعته من خلال العظام من أجل حساب كثافة العظام.
العملية سريعة وبسيطة ، فقط خمس دقائق. :
أنت ترقد على سرير خاص بينما يمر الماسح الضوئي فوق جسمك.

و هذه التكنولوجيا يمكن أن تقيس كثافة العظام في أي بقعة في الجسم، ولكن عادة ما تستخدم لقياس ذلك في العمود الفقري القطني (في أسفل الظهر)، الورك الكلي (موقع معين في الورك بالقرب من مفصل الورك)، والعنق الفخذي (الجزء العلوي من الفخذ، أو عظم الفخذ).
والقراءة تعطي لك معدل T لديك و هي مقارنة بينك و بين متوسط القراءة عند الالاف الطبيعين عند عمر الثلاثين من الأمريكان طبعا الذين تمت الدراسة عليهم .. ولكن اذا كن هناك اختلف بين العرق والجنس واللون و العمي فنأخذ أيضا بمعيار Z و هو مقارنة بينك و بين الآلاف الطبيعيين ممن هم في مثل عمرك


ديكسا ينجز هذا مع عشر واحد فقط من التعرض للإشعاع من الأشعة السينية التي نفوم بها في حال أشعة الصدر، وهو يعتبر المعيار الذهبي لفحص هشاشة العظام، على الرغم من وجود أجهزة الموجات فوق الصوتية، والذي يمكن أن يستخدم م لقياس كثافة المعادن في العظام في ال كعب، أو الذقن ، أو حتى في الإصبع، و في بعض الأحيان يستخدم أيضا في بعض المراكز الصحية الطبية.
من من ملاحق دراسات هارفارد بتصرف
Calcium and vit D
Although bone-weakening osteoporosis is quite common among older people, it isn’t an inevitable part of aging. There’s a lot you can do to shield your bones from this disease.
The best insurance against osteoporosis is building the highest bone density possible by your 30s and minimizing bone loss after that. But if you you’re already in midlife or beyond, there is still much you can do to preserve the bone you have and perhaps even to replace lost bone. Daily weight-bearing exercise, like walking, is the best medicine. Getting enough calcium and vitamin D are two other critical strategies for keeping bones strong.
Calcium
Calcium is an important nutrient for building bone and slowing the pace of bone loss. But it’s not a single magic bullet, and some scientists suggest that too much calcium or dairy products may be unhealthy. Keep in mind that in addition to calcium, there are other nutrients and foods that help keep your bones strong — most importantly vitamin D, but also vitamin K.
How much calcium? The recommended daily intake for calcium is 1,000 milligrams (mg) a day for adults up through age 50 and 1,200 mg a day for people ages 51 and older, when bone loss accelerates. With age, the intestines absorb less calcium from the diet, and the kidneys seem to be less efficient at conserving calcium. As a result, your body can steal calcium from bone for a variety of important metabolic functions.
Ideally, you should get your calcium through dietary sources. Some research suggests that getting too much calcium from supplements may increase the risk of heart disease and prostate cancer. Therefore it’s best to talk with your doctor if you think you need a calcium supplement.
Vitamin D
In building bone, calcium has an indispensable assistant: vitamin D. This vitamin helps the body absorb calcium, and some researchers think that increasing vitamin D can help prevent osteoporosis. Milk sold in the United States is fortified with vitamin D. Vitamin D is also prevalent in fortified breakfast cereals, eggs, and vitamin supplements. Some brands of yogurt are fortified with it, as well as some juices.
If possible, a small amount of sun exposure can help your body manufacture its own vitamin D — about five to 30 minutes of sunlight between 10 a.m. and 3 p.m. twice a week to your face, arms, legs, or back without sunscreen will enable you to make enough of the vitamin. People with fair skin that burns easily should protect themselves from skin cancer by limiting sun exposure to 10 minutes or less.
Food and sun exposure should suffice, but if not, some experts advise getting 1,000 IU of vitamin D daily from a supplement.